Mounjaro Plateau: Strategies That Work

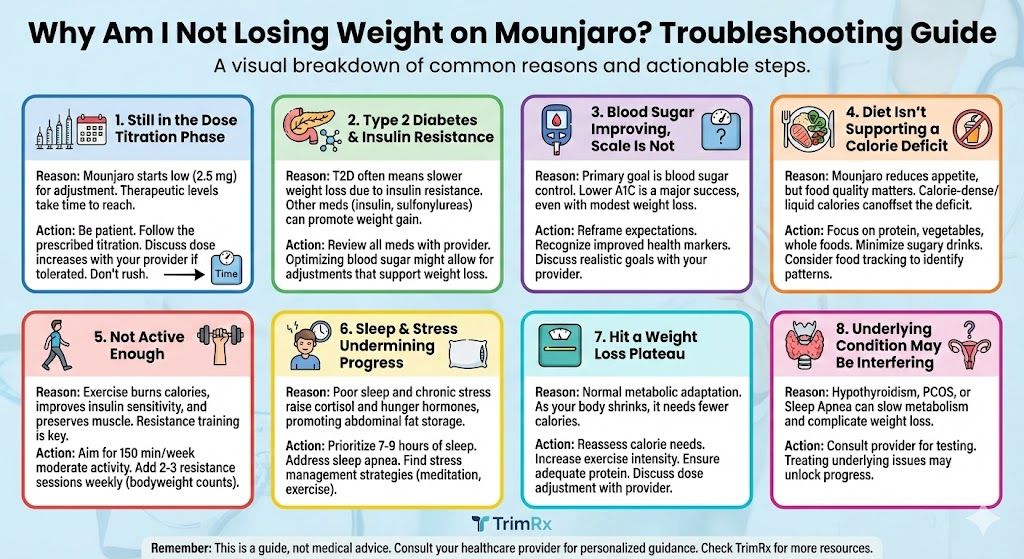
A Mounjaro plateau is when your weight loss stalls for four or more consecutive weeks despite staying consistent with your medication and general routine. If you’ve hit this point, you’re not alone. Plateaus are a normal part of GLP-1 treatment, not a sign that Mounjaro has stopped working. Your body is adapting to its new, lower weight, and the calorie deficit that was driving your initial results has likely narrowed or disappeared entirely. The fix usually involves a combination of dose adjustment, dietary recalibration, and strategic lifestyle changes.
Here’s what’s actually happening and how to push past it.
Why Plateaus Happen on Mounjaro
Your body doesn’t want to lose weight. From an evolutionary standpoint, your metabolism treats fat loss as a potential threat and responds with a series of adaptations designed to slow it down. This is called metabolic adaptation, and it happens regardless of how you’re losing weight.
When you weigh less, you burn fewer calories at rest. Your basal metabolic rate drops roughly proportionally to your body mass. A person who has lost 30 pounds simply needs fewer calories to exist than they did at their higher weight. On top of that, your body becomes slightly more efficient at using the calories you give it. Hormones that regulate hunger (ghrelin) tend to increase, while hormones that signal fullness (leptin) decrease relative to your new body composition.
So the calorie deficit that produced steady two-pound-per-week loss four months ago may now be a calorie deficit of nearly zero. You’re eating the same amount, but your body’s needs have shrunk to match. The result: the scale stops moving.
This isn’t Mounjaro failing. It’s your body doing exactly what it’s designed to do.
Strategy 1: Talk to Your Provider About a Dose Increase
This is the most straightforward plateau breaker and should usually be your first move. Mounjaro’s dosing ranges from 2.5 mg up to 15 mg, and the clinical data shows a clear dose-response relationship. Higher doses produce greater appetite suppression, improved insulin sensitivity, and more weight loss on average.
The SURMOUNT-1 trial published in the New England Journal of Medicine demonstrated that participants on 15 mg of tirzepatide lost over 20% of body weight on average, compared to roughly 15% on 5 mg (Jastreboff et al., NEJM, 2022). If you’ve been sitting at the same dose for more than four weeks and your side effects are manageable, stepping up may reignite your progress.
Your provider can evaluate whether an increase is appropriate based on your tolerability and overall trajectory. If you’ve already discussed dosing before, the Mounjaro first month expectations article covers how the titration process typically unfolds.
Strategy 2: Recalibrate Your Calories
This is the strategy people most often resist, but it’s frequently the one that matters most. The amount of food that created a deficit at your starting weight is not the same amount that creates a deficit at your current weight. Period.
Let’s say a patient started Mounjaro at 230 pounds. At that weight, eating 1,500 calories a day created a solid 500-calorie daily deficit, producing about a pound of loss per week. After losing 30 pounds, their daily maintenance needs have dropped to roughly 1,600 calories. Now that same 1,500-calorie intake only creates a 100-calorie deficit, which is too small to produce visible weekly changes on the scale.
You have two options. Reduce your intake further (which is hard to sustain and not always advisable), or increase your calorie expenditure through activity. Most people do best with a combination of both: a modest calorie adjustment of 100 to 200 fewer calories plus more movement.
Track your food for a week if you haven’t recently. Your actual intake may surprise you. Portion sizes have a way of drifting upward over time without you noticing, especially as your body adapts to the medication’s appetite-suppressing effects.
Strategy 3: Prioritize Protein
Protein does three things that are directly relevant to breaking a plateau. First, it has the highest thermic effect of any macronutrient, meaning your body burns more calories digesting protein than it does digesting carbs or fat. Second, it helps preserve lean muscle mass during weight loss, which protects your metabolic rate. Third, it keeps you fuller for longer, which makes maintaining a calorie deficit easier.
Aim for at least 0.7 grams of protein per pound of your current body weight. For a 200-pound person, that’s about 140 grams daily. Good sources include chicken, turkey, fish, eggs, Greek yogurt, cottage cheese, and lean beef. If hitting that target through food alone is difficult, a protein shake can fill the gap.
Most people on GLP-1 medications undereat protein because their overall appetite is suppressed and they tend to reach for whatever is convenient or appealing. Making protein the anchor of every meal is one of the most impactful changes you can make during a plateau.
Strategy 4: Add or Increase Resistance Training
If you’re not doing any resistance training, starting now is one of the best things you can do for your plateau. If you are doing some, it might be time to increase the intensity or frequency.
Here’s why this matters so much. During weight loss, your body doesn’t just burn fat. It also breaks down muscle for energy, especially if you’re in a significant calorie deficit and not providing enough stimulus for your muscles to stick around. Every pound of muscle you lose reduces your resting metabolic rate by roughly six calories per day. That adds up. Losing 10 pounds of muscle over the course of treatment means your body burns about 60 fewer calories daily at rest, or roughly six pounds less fat burned per year.
Resistance training sends a signal to your body that your muscles are needed and should be preserved. Two to three sessions per week of compound movements (squats, deadlifts, rows, presses, lunges) is enough for most people. You don’t need fancy equipment. Bodyweight exercises, resistance bands, or basic dumbbells all work.
The Mounjaro 3-month results show that patients who combined medication with consistent exercise saw stronger and more sustained outcomes compared to those who relied on the drug alone.
Strategy 5: Increase Daily Movement Outside the Gym
Structured exercise matters, but so does your general daily activity level. NEAT (non-exercise activity thermogenesis) refers to all the calories you burn through movement that isn’t formal exercise: walking, cleaning, fidgeting, taking the stairs, standing instead of sitting.
NEAT actually accounts for a larger portion of most people’s daily calorie burn than their gym sessions. And here’s the problem: when you’re in a calorie deficit, NEAT tends to decrease unconsciously. You move less throughout the day without realizing it. You sit more. You take the elevator instead of the stairs. Your body subtly conserves energy.
Counteracting this is simple in concept: move more during your day. Set a step target of 7,000 to 10,000 steps daily. Take walking meetings. Park farther away. Stand up every hour. These small additions can collectively burn an extra 200 to 300 calories a day, which is often enough to restart a stalled deficit.
Strategy 6: Fix Your Sleep
Poor sleep doesn’t just make you tired. It actively undermines fat loss through hormonal disruption. Sleep deprivation raises ghrelin (hunger hormone), lowers leptin (fullness hormone), elevates cortisol (stress and fat-storage hormone), and increases cravings for high-carb, high-fat foods. This hormonal cocktail can partially override what Mounjaro is doing to your appetite signaling.
If you’re consistently sleeping fewer than seven hours, this could be a meaningful contributor to your plateau. Prioritize sleep hygiene: consistent bedtime, cool and dark room, no screens for 30 minutes before bed, caffeine cutoff by early afternoon. These aren’t flashy strategies, but they work.
Strategy 7: Rule Out Medical and Medication Factors
If you’ve implemented the strategies above and your plateau persists beyond six to eight weeks, it’s time to look at medical factors. Request bloodwork to check thyroid function (TSH), fasting glucose, fasting insulin, and HbA1c. Hypothyroidism, worsening insulin resistance, or other metabolic conditions can develop or progress during treatment and silently stall your results.
Also review your full medication list. Corticosteroids, certain antidepressants, beta-blockers, gabapentin, and insulin or sulfonylureas can all promote weight gain. If you’ve started or increased any of these during your Mounjaro treatment, they could be the hidden brake on your progress.
When to Consider a Different Approach
If you’ve maxed out at 15 mg, optimized nutrition, added strength training, fixed your sleep, and ruled out medical causes, and you’re still stuck, it may be worth exploring compounded options that offer more precise dosing flexibility. TrimRx provides access to compounded tirzepatide, which can offer dosing options and price points that work better for some patients during long-term treatment.
A plateau isn’t a dead end. It’s a signal that something in your approach needs adjusting. Work through these strategies systematically, and most people find that the scale starts moving again within a few weeks.
This information is for educational purposes and is not medical advice. Consult with a healthcare provider before starting any medication. Individual results may vary.
Transforming Lives, One Step at a Time
Keep reading

Mounjaro Cost at Costco in 2026: Real Pricing Breakdown
Without insurance, Mounjaro at Costco costs roughly $1,040 to $1,100 a month for a 28-day supply of four pens in 2026, among the lower…

Mounjaro Cost on GoodRx: Price Breakdown for 2026
With a GoodRx coupon, Mounjaro costs roughly $990 to $1,100 a month in 2026, depending on the pharmacy. That’s only modestly below Eli Lilly’s…

Stopping Mounjaro Gradually vs All at Once: What Works Better
If you are getting ready to stop Mounjaro, one of the first decisions that comes up is whether to step down the dose gradually…

