Ozempic to Mounjaro: Making the Transition

Switching from Ozempic to Mounjaro means moving from a GLP-1 receptor agonist (semaglutide) to a dual GIP/GLP-1 receptor agonist (tirzepatide). Unlike switching between two brands of the same molecule, this is a genuine medication change. You’re adding a second hormonal pathway to your treatment. For many patients, that translates to stronger appetite suppression, improved metabolic effects, and greater total weight loss. The transition itself is straightforward, with no washout period required, though your provider will need to determine the right starting dose on Mounjaro based on where you are in your Ozempic treatment.
Here’s what the switch looks like from start to finish.
Why People Move from Ozempic to Mounjaro
The most common reason is that Ozempic has stopped producing results. You titrated up through the doses, saw good weight loss initially, and then hit a wall. You’ve optimized your diet, added exercise, addressed sleep, and the scale still won’t move. When you’ve genuinely exhausted the options within semaglutide’s framework, switching to a medication with a different mechanism is the logical next step.
Mounjaro’s dual receptor activity gives your body something new to respond to. GIP receptor activation influences fat metabolism, insulin secretion, and appetite regulation through pathways that GLP-1 alone doesn’t fully address. This is why patients who plateau on Ozempic often see renewed progress after switching, even when both medications are technically in the same drug class.
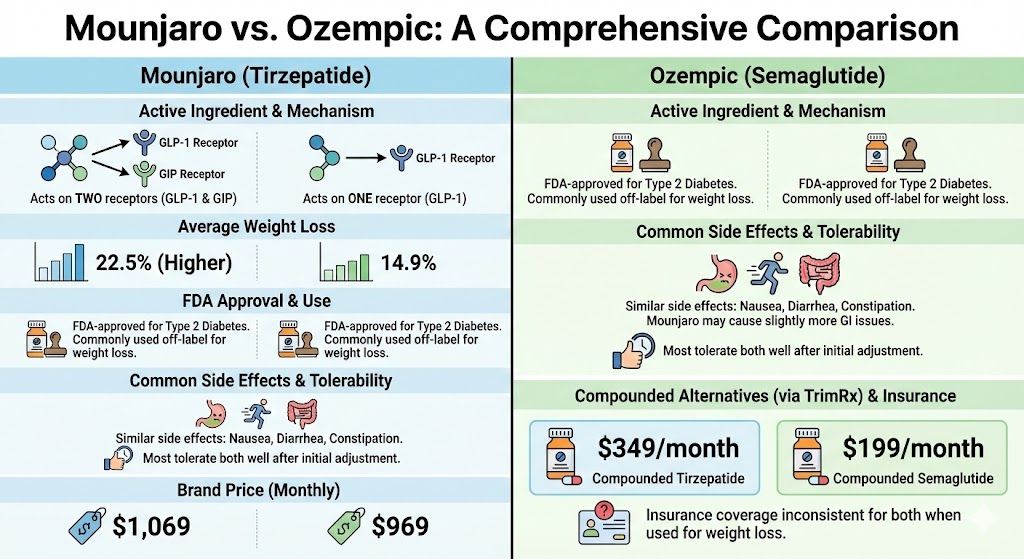
The second reason is stronger clinical data. The SURMOUNT-1 trial (Jastreboff et al., NEJM, 2022) showed tirzepatide at 15 mg produced average weight loss exceeding 22% of body weight. Semaglutide’s best showing in the STEP trials was roughly 15% at 2.4 mg. That’s a meaningful gap, and for patients with a significant amount of weight to lose, that extra efficacy matters.
The third reason is side effect differences. While both medications share similar GI side effect profiles, individual responses vary. Some patients who experience persistent nausea or GI distress on semaglutide find that tirzepatide is easier to tolerate, or the reverse. The only way to know is to try.
Cost can also factor in. Depending on insurance coverage, copay programs, and whether compounded options are being considered, one medication may be substantially more affordable than the other. TrimRx offers both compounded semaglutide and compounded tirzepatide, which can change the cost calculus significantly compared to brand pricing.
How the Two Medications Differ
Understanding what’s changing helps you know what to expect.
Ozempic (semaglutide) activates GLP-1 receptors. This slows gastric emptying, reduces appetite through brain signaling, and improves insulin sensitivity. It’s effective and well-studied, with dosing from 0.25 mg to 2 mg.
Mounjaro (tirzepatide) activates both GLP-1 and GIP receptors. It does everything Ozempic does through the GLP-1 pathway, plus adds GIP-mediated effects on fat metabolism, glucose regulation, and appetite. Dosing ranges from 2.5 mg to 15 mg.
These are different molecules with different receptor profiles, so the doses aren’t interchangeable or directly comparable. Ozempic 1 mg doesn’t equal Mounjaro 1 mg. Your provider determines the appropriate Mounjaro starting dose based on your current Ozempic dose, how long you’ve been on it, and your overall treatment response.
The injection schedule is the same for both: once weekly, subcutaneous, on the same day each week. Injection technique is identical. The pens look and feel slightly different, but the process is the same.
How the Transition Works
The switch is a simple one-for-one replacement on your weekly injection schedule. No washout period is needed. Semaglutide and tirzepatide don’t interact with each other, and your body doesn’t need time to clear one before starting the other.
The standard approach: take your last Ozempic injection on your regular day, then start Mounjaro the following week on that same day.
The starting dose on Mounjaro depends on where you were with Ozempic:
If you were on Ozempic 0.25 mg or 0.5 mg, you’ll typically start Mounjaro at 2.5 mg. This is the standard onboarding dose, and since your GLP-1 exposure has been relatively low, your provider will likely follow the normal titration from the beginning.
If you were on Ozempic 1 mg, most providers start Mounjaro at 2.5 mg or 5 mg. Starting at 5 mg is reasonable here because your body has established tolerance to GLP-1 activity, and 2.5 mg may feel like a significant step backward in appetite suppression.
If you were on Ozempic 1.5 mg or 2 mg, starting at Mounjaro 5 mg is the most common approach. Some providers will go directly to 7.5 mg for patients who were on maximum-dose Ozempic with good tolerability, though this is less standard.
There’s no universally agreed-upon conversion chart. These are guidelines, and your provider makes the final call based on your individual situation. The goal is to maintain adequate appetite suppression during the transition without overwhelming your system with a dose that’s too high.
What the First Few Weeks Feel Like
Most patients describe the transition as noticeable but manageable. You’re introducing a new receptor pathway (GIP) that your body hasn’t encountered in this therapeutic context before, so there’s a brief adjustment period.
Common experiences during weeks one and two:
Appetite suppression feels different. Many patients describe it as broader or more consistent. On Ozempic, appetite suppression often centers around feeling full quickly during meals (a gastric emptying effect). On Mounjaro, patients frequently report less interest in food between meals as well, which may reflect the added GIP activity. The quality of the suppression changes, not just the intensity.
GI side effects may temporarily resurface. Even with established GLP-1 tolerance from Ozempic, the GIP component is new. Mild nausea, slight changes in bowel patterns, or occasional bloating during the first week or two is common. These effects are typically less intense than what you experienced when first starting Ozempic, since one pathway is already familiar.
Consider this scenario: a patient switches from Ozempic 2 mg to Mounjaro 5 mg. During the first week, they notice mild nausea on day two that resolves by day three, slightly reduced appetite compared to their last few weeks on Ozempic, and one day of looser stools. By week two, GI symptoms have cleared and appetite suppression feels noticeably stronger than what they’d been experiencing on Ozempic. This is a very typical transition experience.
Energy levels generally remain stable. Some patients report feeling slightly more energetic within the first few weeks, possibly related to improved glucose regulation from the dual mechanism.
When Weight Loss Resumes After Switching
If you’re switching because of an Ozempic plateau, set realistic expectations for the first few weeks. Starting Mounjaro at 2.5 mg or 5 mg is likely a lower effective dose than where you ended on Ozempic. Your body needs time to titrate up to the dose range where Mounjaro’s full effect kicks in.
Most patients who switch from Ozempic start seeing renewed weight loss within four to eight weeks, typically coinciding with reaching the 7.5 mg or 10 mg dose level. The Mounjaro first month article covers what to expect during the early dose escalation phase.
By the three-month mark on Mounjaro, most patients who switched from Ozempic are seeing clear, consistent progress. The Mounjaro 3-month results provide benchmarks, though keep in mind that patients switching from another GLP-1 may have a slightly different trajectory than those starting Mounjaro as their first medication.
The key is patience during the titration phase. The early weeks at lower doses may feel frustrating if you’re eager for results, but the clinical data strongly supports the payoff at higher doses.
Managing Side Effects During the Switch
The side effect profile of Mounjaro is similar to Ozempic: nausea, diarrhea or constipation, decreased appetite, and occasional injection site reactions. Your established GLP-1 tolerance from Ozempic means you’ll likely experience milder versions of these compared to a GLP-1 naive patient.
Practical strategies that help:
Eat smaller, more frequent meals during the first two weeks. Large meals are harder to tolerate when gastric emptying is slowed, and the adjustment to the GIP pathway can temporarily increase sensitivity. Prioritize protein and reduce high-fat, greasy foods during the transition. Fat slows digestion further and tends to worsen nausea. Stay hydrated. Both GLP-1 and GIP activity can affect fluid balance, and dehydration amplifies nausea and constipation. Time your injection for when mild nausea would be least disruptive. Many patients prefer Thursday or Friday evening so any first-day queasiness falls on the weekend.
If side effects are more than mild, let your provider know. They may recommend staying at your current dose for an extra week or two before the next increase, which usually resolves the issue.
The Cost Question
Brand-name Mounjaro and Zepbound (Eli Lilly’s weight-loss-indicated version of tirzepatide) both carry list prices above $1,000 monthly without insurance. If you were paying cash for Ozempic, you may find tirzepatide pricing similar or slightly different depending on dose and pharmacy.
Insurance coverage depends on your plan and your diagnosis. If you have type 2 diabetes, Mounjaro is often the easier product to get covered. If your primary indication is weight management without diabetes, Zepbound may be the better insurance fit, since it’s FDA-approved for that purpose.
If insurance coverage is a barrier for either product, compounded tirzepatide offers a way to access the same active ingredient without navigating formulary restrictions. TrimRx’s compounded tirzepatide includes provider consultation, prescription, and home delivery at a fraction of brand cost.
Is the Switch Right for You?
Moving from Ozempic to Mounjaro makes strong clinical sense if you’ve plateaued on semaglutide at or near maximum dose, if your appetite suppression has faded and dose increases haven’t restored it, or if you want access to a medication with a higher average weight loss ceiling.
It’s less necessary if you’re still losing weight on Ozempic, still have dose increases available, or haven’t yet addressed lifestyle factors that could be contributing to a stall. The Ozempic plateau article walks through how to determine whether your plateau is dose-related or caused by something else entirely.
If you’re ready to explore the switch, TrimRx’s intake quiz can connect you with a provider who manages these transitions regularly and can build a titration plan tailored to your history and goals.
This information is for educational purposes and is not medical advice. Consult with a healthcare provider before starting any medication. Individual results may vary.
Transforming Lives, One Step at a Time
Keep reading

Ozempic Alternatives: Your Options Compared
If Ozempic isn’t the right fit, whether because of cost, side effects, availability, or results, you have real alternatives. The closest ones are other…

Ozempic vs Wegovy: Same Drug, Different Purpose
Here’s the fact that surprises most people: Ozempic and Wegovy are the same medication (semaglutide), just sold under different brand names, at different doses,…

When Do “Ozempic Vulva” Changes Start and Stabilize? A Timeline
Vulvar and genital changes from GLP-1 weight loss follow the pace of your weight loss, so they typically begin within the first few months…

