What Happens When You Stop Taking Semaglutide?

When you stop taking semaglutide, the appetite suppression fades within a few weeks, and most people regain a significant portion of their lost weight over the following six to twelve months. Research from the STEP 1 extension study showed approximately two-thirds of weight lost was regained within a year of stopping. This happens because semaglutide treats the symptoms of a chronic condition, and when treatment stops, those symptoms return.
If you’re reading this, you’re probably either thinking about stopping, have already stopped, or had your supply interrupted. Whatever brought you here, the goal is to give you a realistic picture of what to expect and practical guidance for whatever comes next.
How Semaglutide Works (And Why Stopping Matters)
Semaglutide mimics GLP-1, a hormone your gut naturally produces after eating. GLP-1 tells your brain you’re full, slows the rate food leaves your stomach, and helps regulate insulin release. In people with obesity, this signaling system is often insufficient to prevent overeating. Semaglutide amplifies it.
The medication also acts directly on appetite centers in the hypothalamus, reducing what patients commonly call “food noise,” the persistent mental preoccupation with eating. This effect is often described as the most life-changing part of treatment, even more than the weight loss itself.
When semaglutide leaves your system, both of these mechanisms shut down. Your gut signals weaken to their pre-medication level, and the hypothalamic effects disappear. The food noise comes back. Hunger returns to its original intensity. Gastric emptying speeds up. And your body, which has been defending a new lower weight while the medication held the line, begins pushing toward regain.
This isn’t the medication “wearing off” in a problematic sense. It’s the condition it was treating reasserting itself, just as blood pressure rises when you stop an antihypertensive.
The Discontinuation Timeline
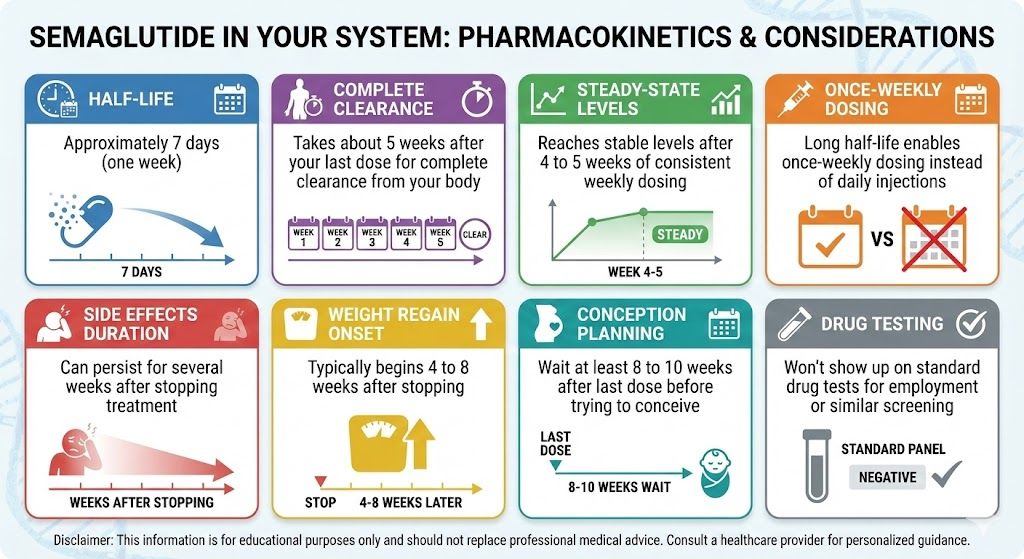
Semaglutide’s half-life is about seven days, which means it takes five to seven weeks after your last injection for the drug to fully clear your body. The transition happens in stages.
Weeks one through two feel largely unchanged. Enough medication remains in your system to maintain most of its effects. Appetite stays suppressed, portions still feel adequate, and the mental quiet around food persists.
Weeks three through four bring the first noticeable shifts. Hunger between meals starts increasing. You might find yourself thinking about food more often, not obsessively, but in a way that feels different from the past several months. Meals that used to be completely satisfying might leave you wanting a little more.
Weeks five through seven mark the full transition. Appetite is back to baseline. The food noise has returned. Gastric emptying has normalized, so fullness after meals doesn’t last as long. Your body is operating without GLP-1 support for the first time since you started treatment.
By months two and three, the weight trajectory becomes clear. The scale starts moving upward for most people. Not dramatically at first, maybe a pound or two per week, but consistently enough that the trend is unmistakable.
The semaglutide timeline during active treatment shows a predictable downward curve. The timeline after stopping shows an almost mirror-image climb back up, though regain often happens somewhat faster than the original loss.
What the Data Tells Us
The STEP 1 extension, published by Wilding et al. in Diabetes, Obesity and Metabolism (2022), tracked participants after they stopped semaglutide following 68 weeks of treatment. The average weight regain was approximately two-thirds of total weight lost within one year of discontinuation.
But the study revealed something equally important: it wasn’t just weight that came back. Improvements in blood pressure, waist circumference, C-reactive protein (an inflammatory marker), and lipid levels all deteriorated as weight returned. The metabolic benefits of treatment reversed alongside the weight regain.
This is a point worth sitting with. Semaglutide doesn’t just make you lighter. It makes you metabolically healthier. Stopping the medication puts both of those outcomes at risk.
The STEP 5 trial provides the contrast. Participants who remained on 2.4 mg semaglutide for 104 weeks maintained their weight loss throughout. The weight that stabilized around week 60 held steady through the end of the study. Continued treatment worked. Discontinuation didn’t.
Not every individual follows the average. Some people regain less, particularly those who made significant behavioral changes during treatment and had less weight to lose initially. But relying on being the outlier isn’t a reliable strategy.
Physical and Psychological Effects of Stopping
The physical changes after stopping semaglutide go beyond the scale.
Appetite intensity is the most immediate and disruptive change. On semaglutide, hunger feels manageable, almost polite. Off semaglutide, it can feel relentless. The hormonal drivers of hunger, particularly ghrelin, increase after weight loss, and without semaglutide counteracting them, those signals hit full force. Many people describe the return of appetite as the single hardest part of stopping.
Digestive patterns change. Semaglutide slows gastric emptying significantly, which is part of why you feel full for hours after a modest meal. Once the medication clears, your stomach empties at its normal pace. Meals that lasted you five or six hours might leave you hungry in three. The practical result is more frequent eating, more snacking, and larger portions, all of which drive caloric intake upward.
Blood sugar stability decreases. Even in non-diabetic patients, semaglutide smooths out glucose fluctuations. Without it, you may notice more energy highs and lows throughout the day, particularly the mid-afternoon crash that tends to trigger carbohydrate cravings.
GI side effects resolve completely. Nausea, constipation, and sulfur burps disappear as the medication leaves your system. If side effects were a significant burden for you, this is a genuine relief.
The psychological impact often surprises people. Months of relative peace around food, of not thinking constantly about meals and snacks and cravings, creates a new normal. When that peace lifts, it can feel like losing something fundamental. Some patients describe grief, frustration, or a sense of failure that compounds the physical changes. These reactions are normal and don’t reflect any personal shortcoming. They reflect the reality of losing a tool that was making an incredibly hard thing much more manageable.
Reasons People Stop (And What to Do Instead)
Cost is the primary driver. Brand-name semaglutide (whether Wegovy or Ozempic) runs $900 to $1,300 or more per month without insurance. Coverage varies wildly between plans, and even insured patients face prior authorizations and potential coverage gaps. If cost is forcing your hand, compounded semaglutide through TrimRx offers the same medication at a substantially lower price. Switching to a compounded formulation keeps you on treatment without the insurance headaches.
Side effects that persist beyond dose escalation push some patients to quit. Before stopping entirely, discuss dose reduction with your provider. Dropping from 2.4 mg to 1.7 mg or 1.0 mg often resolves persistent GI issues while still providing appetite support that’s far better than nothing.
Reaching a goal weight creates the temptation to stop. The logic feels sound: the problem is solved, why keep taking medicine? But the data on long-term semaglutide use makes clear that the medication is what’s maintaining the solution. Obesity is chronic. Treatment should be too, for most people.
Wanting to try a different approach is reasonable. If semaglutide isn’t giving you the results you want, switching to tirzepatide can be more productive than stopping GLP-1 therapy altogether. Tirzepatide’s dual mechanism produces greater average weight loss, and some people who plateau on semaglutide respond well to the switch.
Pregnancy planning requires stopping. Semaglutide should be discontinued at least two months before attempting to conceive. Plan this transition with your provider so it’s structured rather than abrupt.
If You Must Stop: Doing It Right
A tapered approach helps. Step down through the lower doses (1.7 mg, 1.0 mg, 0.5 mg, 0.25 mg) over several weeks rather than going from your full dose to nothing. This gives your appetite regulation a more gradual transition instead of a sharp cliff.
Build your behavioral foundation while you still have medication support. High-protein eating patterns, consistent resistance training, structured meal timing, and good sleep habits all provide a buffer against regain. They won’t prevent it entirely for most people, but they can slow the pace and limit the total amount.
Set a clear monitoring plan. Weekly weigh-ins, same conditions each time. Define a regain threshold with your provider, say ten pounds above your lowest weight, that triggers a re-evaluation. Having a plan prevents the slow drift of “I’ll deal with it next month” that allows significant regain to accumulate.
Protect your mental health. Consider therapy or a support community during the transition. The emotional weight of watching progress reverse is real and deserves attention, not dismissal.
The Bigger Picture
Stopping semaglutide doesn’t have to mean stopping treatment. If your current formulation, dose, or provider isn’t working, there are options. Compounded versions, alternative medications, dose adjustments, and different GLP-1 medications all exist precisely because one size doesn’t fit everyone.
The worst outcome isn’t needing to change your approach. It’s abandoning treatment entirely and losing the health gains you worked to build. Whatever challenge is making you consider stopping, there’s likely a path that keeps you on some form of therapy while addressing the specific problem.
If you’re weighing your options or need a provider who can help you plan your next step, take the intake quiz to connect with a TrimRx clinician who specializes in GLP-1 weight management.
This information is for educational purposes and is not medical advice. Consult with a healthcare provider before starting any medication. Individual results may vary.
Transforming Lives, One Step at a Time
Keep reading

Semaglutide vs Orforglipron: How the Two GLP-1 Options Compare
Semaglutide and orforglipron are both GLP-1 receptor agonists, but they differ in chemistry, delivery, and daily routine. Semaglutide is a peptide, available as a…

What Is CagriSema? The Semaglutide-Amylin Combination Explained
CagriSema is an investigational once-weekly injection from Novo Nordisk that combines two drugs in a single shot: semaglutide (the GLP-1 medication in Wegovy and…

Retatrutide vs Semaglutide: What’s Different
Semaglutide is the GLP-1 medication most people have heard of, sold as Ozempic and Wegovy and now available as a once-daily pill too. It’s…

