GLP-1 and Hormones: What Women Need to Know Before Starting Treatment

Women’s hormonal systems are more complex than a simple calorie-in, calorie-out model accounts for, and when you introduce a medication that fundamentally alters appetite signaling and metabolic function, the interactions with that hormonal complexity deserve attention. GLP-1 medications like semaglutide and tirzepatide have become widely used among women for weight loss, but the conversation around how they interact with estrogen, insulin, the menstrual cycle, thyroid function, and fertility is still catching up to the pace of prescribing.
The short answer: GLP-1 medications are generally safe for women across reproductive life stages, but there are specific hormonal interactions and considerations that are worth understanding before you start. Here’s what the current evidence shows.
How GLP-1 Medications Work and Why Hormones Are Relevant
GLP-1 (glucagon-like peptide-1) is itself a hormone, produced in the gut in response to food intake. It signals the brain to reduce appetite, stimulates insulin secretion from the pancreas, suppresses glucagon, and slows gastric emptying. GLP-1 receptor agonist medications like semaglutide and tirzepatide mimic and extend these effects far beyond what the body produces naturally.
Because GLP-1 is a hormone that interacts with insulin, glucose metabolism, and appetite regulation systems, introducing it pharmacologically doesn’t happen in isolation. It touches systems that also respond to estrogen, progesterone, cortisol, and thyroid hormones. Understanding these intersections helps women anticipate what they might experience during treatment and why.
GLP-1 and Insulin: The Most Direct Hormonal Connection
The relationship between GLP-1 medications and insulin is the most well-established hormonal interaction. GLP-1 receptor agonists stimulate glucose-dependent insulin secretion, meaning they prompt the pancreas to release insulin when blood sugar rises after eating. This is why these medications are effective for type 2 diabetes management alongside weight loss.
For women with insulin resistance, which is common in polycystic ovary syndrome (PCOS), prediabetes, and obesity, this effect is particularly meaningful. Improving insulin sensitivity can have downstream effects on other hormonal systems. In women with PCOS, for example, elevated insulin levels drive excess androgen production, contributing to irregular periods, excess hair growth, and acne. Reducing insulin resistance through GLP-1 therapy can partially address these androgenic effects, which is part of why GLP-1 medications have attracted interest in the PCOS community.
For a deeper look at this specific application, the GLP-1 for PCOS overview covers the evidence and clinical considerations in detail.
Effects on the Menstrual Cycle
Women starting GLP-1 medications sometimes notice changes in their menstrual cycle, particularly in the first few months of treatment. These changes are generally indirect rather than a direct pharmacological effect of semaglutide or tirzepatide on reproductive hormones.
The most common pathway is through weight loss itself. Significant weight loss, particularly rapid weight loss, can temporarily disrupt the hypothalamic-pituitary-ovarian (HPO) axis, the hormonal feedback loop that regulates ovulation and menstruation. This can produce irregular cycles, missed periods, or changes in cycle length and flow, particularly in women who lose weight quickly in the early months of treatment.
For women with PCOS who had irregular cycles before starting treatment, GLP-1 therapy sometimes produces the opposite effect: improved cycle regularity as insulin resistance decreases and androgen levels normalize. This is worth knowing because improved ovulatory function also means improved fertility, which leads directly to the next consideration.
Fertility and Contraception: A Critical Conversation
GLP-1 medications are not recommended during pregnancy, and Wegovy’s prescribing information specifically recommends stopping the medication at least two months before a planned pregnancy. This is relevant for women of reproductive age who are using GLP-1 therapy for weight loss.
Here’s where the hormonal interaction becomes practically important: if weight loss on GLP-1 therapy improves ovulatory function, particularly in women with PCOS or obesity-related anovulation, fertility may increase during treatment even if cycles were previously irregular or absent. Women who were not actively protecting against pregnancy because they assumed they were unlikely to conceive need to factor this in.
Additionally, semaglutide may reduce the absorption of oral contraceptive pills by slowing gastric emptying. The clinical significance of this effect is not fully characterized, but some providers recommend that women on oral contraceptives switch to a non-oral method (patch, ring, IUD, implant) when starting GLP-1 therapy, or use backup contraception during the titration period. This is worth discussing explicitly with your prescribing provider.
Thyroid Hormone Interactions
The relationship between GLP-1 medications and thyroid function is one of the more discussed topics in this space, and it’s worth addressing clearly. GLP-1 receptor agonists have been shown in rodent studies to stimulate C-cell growth in the thyroid, which raised initial concerns about thyroid cancer risk. This is why these medications carry a black box warning for patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2.
In human studies conducted to date, no increased risk of thyroid cancer has been established, but the warning remains in place given the rodent data and the fact that long-term human data is still accumulating. For women with existing thyroid conditions, such as hypothyroidism managed with levothyroxine, GLP-1 medications don’t directly interact with thyroid hormone replacement. However, the gastric emptying effect of GLP-1 medications can affect levothyroxine absorption timing. Thyroid hormone replacement is typically taken on an empty stomach, and changes in gastric motility can affect absorption consistency. Women on levothyroxine should mention this to their provider when starting a GLP-1 medication.
Estrogen, Body Composition, and Fat Distribution
GLP-1 medications don’t directly alter estrogen levels, but weight loss achieved through GLP-1 therapy can have indirect effects on estrogen metabolism that are worth understanding. Adipose tissue is a site of estrogen production, particularly in postmenopausal women where the ovaries are no longer the primary estrogen source. Significant fat loss can reduce peripheral estrogen production, which may affect symptoms in postmenopausal women not on HRT.
For premenopausal women, the shift in body composition produced by GLP-1 therapy, particularly the reduction in visceral fat, generally improves the hormonal environment rather than disrupting it. Visceral fat is metabolically active in ways that promote inflammation and insulin resistance, both of which have downstream effects on hormonal balance. Reducing visceral fat tends to improve insulin sensitivity, reduce inflammatory markers, and support more stable hormonal signaling overall.
Bone Health During GLP-1 Treatment
Estrogen plays a protective role in maintaining bone mineral density, and both menopause and rapid weight loss can reduce bone density. For women on GLP-1 therapy who are losing weight at a meaningful pace, bone health is worth monitoring, particularly in perimenopausal and postmenopausal women where estrogen-related bone protection is already diminishing.
Practical steps include ensuring adequate calcium and vitamin D intake throughout treatment, incorporating weight-bearing exercise, and discussing bone density monitoring with your provider if you have additional risk factors. This isn’t a reason to avoid treatment, but it’s a variable that deserves attention in a longer-term treatment plan.
Cortisol, Stress, and Appetite Regulation
One underappreciated hormonal interaction involves cortisol. Chronic stress elevates cortisol, which drives appetite, promotes abdominal fat storage, and can blunt the appetite-suppressing effects of GLP-1 medications. Women managing significant stress alongside GLP-1 therapy may find results slower than expected, not because the medication isn’t working, but because the cortisol-driven appetite signal is partially counteracting it.
This doesn’t require a separate medication to address, but it does mean that sleep quality, stress management, and psychological support during treatment aren’t optional extras. They’re part of the metabolic equation.
Accessing GLP-1 Treatment as a Woman
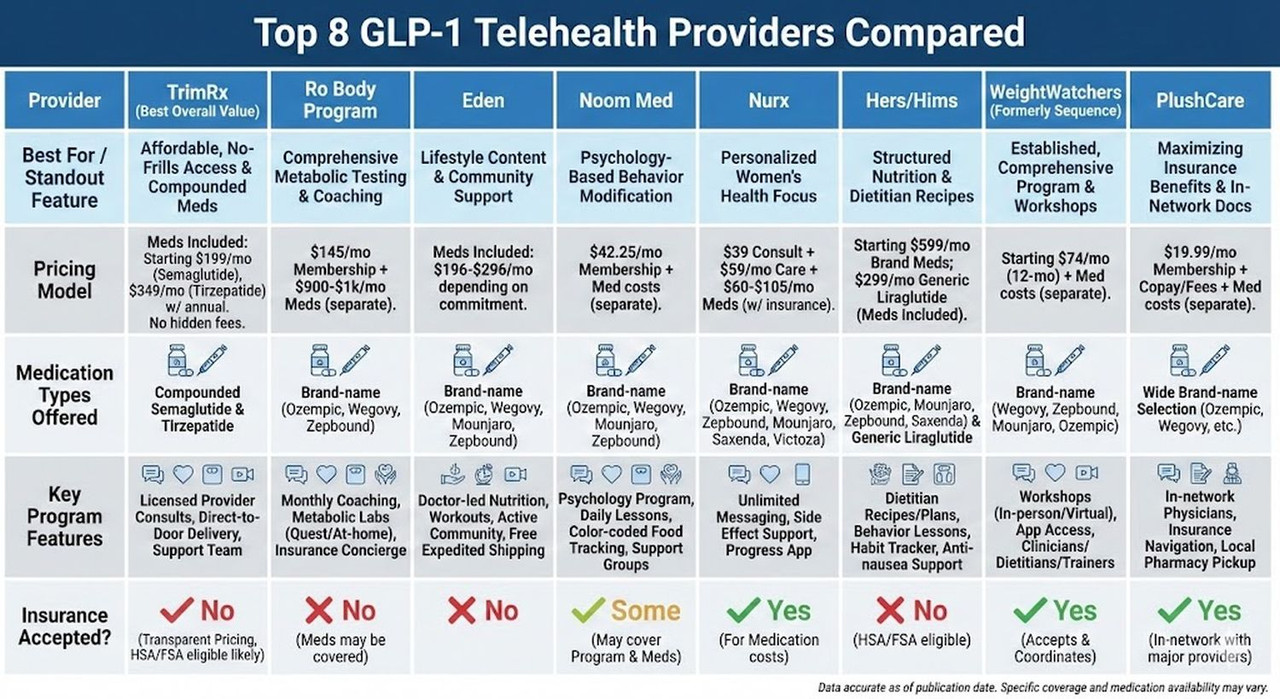
Women across reproductive life stages can access GLP-1 medications through their gynecologist, PCP, endocrinologist, or a telehealth platform. TrimRx offers compounded semaglutide and compounded tirzepatide through a telehealth model that reviews your full health history, including hormonal health considerations, before a provider makes a prescribing decision.
If you want to understand what early treatment typically involves, the semaglutide first week guide covers what most patients experience in the early days of treatment.
To find out whether you’re a candidate, start your eligibility assessment here.
A 2023 study published in the Journal of Clinical Endocrinology and Metabolism found that GLP-1 receptor agonist therapy in women with obesity and insulin resistance produced significant improvements in androgen levels, menstrual regularity, and metabolic markers, with effects most pronounced in women with baseline hyperinsulinemia, underscoring how tightly GLP-1 mechanisms are connected to broader hormonal function in women.
Understanding these interactions doesn’t make the decision to start GLP-1 therapy more complicated. It makes it more informed, which is exactly where good treatment decisions start.
This information is for educational purposes and is not medical advice. Consult with a healthcare provider before starting any medication. Individual results may vary.
Transforming Lives, One Step at a Time
Keep reading

Vegan and GLP-1: Meeting Your Protein Needs Without Animal Products
Going vegan while on a GLP-1 medication is entirely doable, but it requires more nutritional intentionality than either approach demands on its own. Semaglutide…

GLP-1 and Bodybuilding: How to Preserve Muscle Mass While Losing Fat
Bodybuilders and serious lifters approach weight loss differently than most people. Where a general patient might be satisfied losing 20 pounds regardless of composition,…
GLP-1 and Intermittent Fasting: Does the Double Approach Work?
Intermittent fasting has spent the better part of a decade as one of the more popular dietary strategies for weight loss, and for good…

