GLP-1 Medications After 50: What Changes and What to Expect

Weight loss after 50 is genuinely harder than it was at 30, and that’s not a mindset problem. It’s physiology. Metabolism slows, muscle mass declines, hormonal shifts alter how the body stores fat, and the caloric deficit required to produce meaningful weight loss becomes more difficult to sustain through diet and exercise alone.
GLP-1 medications address some of these challenges directly, which is part of why demand for semaglutide and tirzepatide has been particularly strong among adults in their 50s and 60s.
The short answer: GLP-1 medications can work well for adults over 50, but the approach to dosing, monitoring, and supporting your body during treatment needs to account for the physiological realities of this life stage. Here’s what you need to know.
Why Weight Loss Gets Harder After 50
Before getting into the medications themselves, it helps to understand what you’re actually working against.
After 50, most adults experience a combination of factors that make weight management more difficult. Resting metabolic rate continues its gradual decline, meaning the body burns fewer calories at rest than it did in earlier decades. Muscle mass decreases at an accelerating rate, a process called sarcopenia, and since muscle tissue burns more calories than fat tissue, this compounds the metabolic slowdown.
Hormonal changes play a significant role as well. In women, the transition through perimenopause and menopause involves declining estrogen levels that shift fat storage toward the abdomen. In men, declining testosterone after 50 contributes to both muscle loss and increased visceral fat accumulation. These hormonal shifts don’t respond well to caloric restriction alone, which is part of why many adults find that approaches that worked in their 30s simply stop producing results after 50.
GLP-1 receptor agonists work on appetite regulation and metabolic signaling in ways that are largely independent of these hormonal factors, which is why they can be effective even when traditional approaches have stalled.
How GLP-1 Medications Work in This Age Group
GLP-1 medications like semaglutide (the active ingredient in Ozempic and Wegovy) and tirzepatide (Mounjaro and Zepbound) work by mimicking gut hormones that regulate appetite and blood sugar. They slow gastric emptying, increase satiety signals to the brain, and reduce the drive to overeat.
For adults over 50, this mechanism addresses a specific challenge. Appetite regulation becomes less reliable with age, and the hormonal signals that naturally suppress hunger after eating can weaken. GLP-1 medications essentially amplify and extend those satiety signals, making it easier to maintain a caloric deficit without the constant hunger that makes dietary restriction so difficult to sustain.
Tirzepatide has an additional mechanism as a dual GIP and GLP-1 agonist, meaning it activates two separate gut hormone receptors simultaneously. Clinical trials have shown it produces somewhat larger average weight loss than semaglutide alone, which may be relevant for adults over 50 who have more metabolic resistance to overcome. The tirzepatide weight loss results research breaks down what the clinical data actually shows.
What’s Different About Using GLP-1s After 50
The medications themselves work the same way regardless of age. What changes is how you need to support your body during treatment and what risks deserve closer attention.
Muscle Preservation Is the Central Concern
This comes up in every conversation about GLP-1 use in older adults, and it deserves direct attention here too. When the body loses weight on these medications, it loses both fat and lean muscle mass. In a 35-year-old, this is manageable. In a 55-year-old who is already experiencing age-related muscle loss, the stakes are higher.
Muscle loss at this life stage is linked to reduced strength, increased fall risk, metabolic slowdown, and long-term functional decline. The practical response is to prioritize protein intake aggressively during treatment, aiming for at least 1.2 to 1.6 grams of protein per kilogram of body weight per day, well above standard recommendations. Resistance exercise, even moderate resistance training two to three times per week, significantly reduces muscle loss during GLP-1-induced weight loss.
Slower Titration Often Makes Sense
GI side effects like nausea, vomiting, and diarrhea are the most common reason patients reduce their dose or discontinue GLP-1 therapy. For adults over 50, these side effects carry a slightly higher risk of dehydration and electrolyte imbalance than they do in younger patients, particularly if kidney function has begun to decline with age.
Starting low and going slow with dose titration reduces this risk meaningfully. Many providers recommend extending the titration period for patients over 50, spending more weeks at each dose level before stepping up, rather than following the most aggressive standard schedule.
For reference on what standard titration looks like, the starting dose of tirzepatide guide covers what patients typically experience in the early weeks.
Bone Density Deserves Attention
Rapid weight loss at any age can reduce bone mineral density, and this risk is amplified after 50 when bone density is already declining, particularly in postmenopausal women. Patients over 50 starting GLP-1 therapy should discuss bone health monitoring with their provider, ensure adequate calcium and vitamin D intake, and incorporate weight-bearing exercise into their routine. This isn’t a reason to avoid treatment, but it’s a variable worth tracking.
Results: What Adults Over 50 Can Realistically Expect
Clinical trial data on GLP-1 medications generally skews toward younger to middle-aged adult populations, but real-world evidence and subgroup analyses suggest that adults over 50 achieve meaningful weight loss on these medications, though often at a somewhat slower pace than younger patients.
The SURMOUNT-1 trial for tirzepatide showed average weight loss of 15 to 22 percent of body weight across the full study population. Subgroup analyses suggest that older adults and those with more metabolic resistance tend toward the lower end of that range, but 10 to 15 percent body weight reduction over 12 to 18 months is a realistic expectation for many patients over 50.
For adults dealing with a weight loss plateau after initial progress, which is common at this age, the Ozempic plateau guide covers the most common causes and what providers typically recommend.
Which Medication Makes More Sense After 50
Both semaglutide and tirzepatide are viable options. The choice often comes down to individual response, tolerability, and cost.
Tirzepatide’s dual mechanism tends to produce larger average weight loss in clinical trials, which may be an advantage for adults over 50 who face greater metabolic resistance. Semaglutide has a longer track record and more published long-term safety data, which some patients and providers find reassuring.
For patients with type 2 diabetes, either medication addresses both blood sugar management and weight, which is particularly relevant for the over-50 population where type 2 diabetes prevalence is significantly higher.
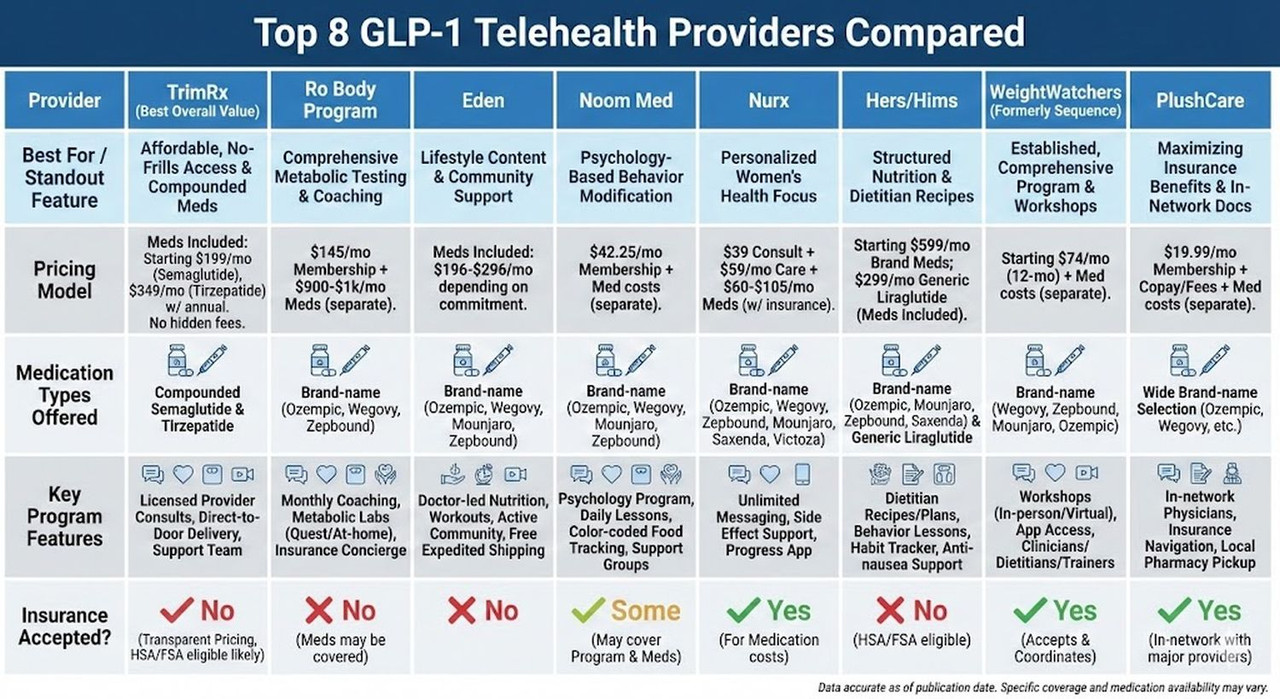
Cost is a practical factor. Brand-name Wegovy and Zepbound list between $900 and over $1,500 per month without insurance. Compounded versions of both active ingredients are available at substantially lower cost through telehealth platforms. TrimRx offers both compounded semaglutide and compounded tirzepatide through a telehealth model that doesn’t require insurance approval.
How to Get Started After 50
The path to starting GLP-1 therapy after 50 runs through a licensed provider who can evaluate your health history, current medications, and baseline labs. Your PCP is a natural starting point if they’re actively managing obesity treatment. If not, telehealth platforms offer a practical alternative.
A 2022 study published in Diabetes, Obesity and Metabolism found that adults over 50 achieved clinically significant weight loss on semaglutide, with cardiovascular and metabolic risk reductions comparable to younger cohorts, though the authors noted the importance of individualized monitoring protocols for older patients given the higher baseline prevalence of comorbidities.
If you want to find out whether you’re a candidate, start your eligibility assessment here. The intake process reviews your health profile and helps determine which medication and approach fits your situation.
The biology of weight loss after 50 is more complicated than it was at earlier life stages. But it’s not hopeless, and for many adults in this age group, GLP-1 therapy provides a meaningful path forward that diet and exercise alone haven’t been able to deliver.
This information is for educational purposes and is not medical advice. Consult with a healthcare provider before starting any medication. Individual results may vary.
Transforming Lives, One Step at a Time
Keep reading

Vegan and GLP-1: Meeting Your Protein Needs Without Animal Products
Going vegan while on a GLP-1 medication is entirely doable, but it requires more nutritional intentionality than either approach demands on its own. Semaglutide…

GLP-1 and Bodybuilding: How to Preserve Muscle Mass While Losing Fat
Bodybuilders and serious lifters approach weight loss differently than most people. Where a general patient might be satisfied losing 20 pounds regardless of composition,…
GLP-1 and Intermittent Fasting: Does the Double Approach Work?
Intermittent fasting has spent the better part of a decade as one of the more popular dietary strategies for weight loss, and for good…

