Oral Tirzepatide: Everything You Need to Know About Oral GLP-1 Options

Oral tirzepatide is not currently available as an FDA-approved medication, but oral semaglutide (Rybelsus) exists as the only FDA-approved oral GLP-1 option for type 2 diabetes, not specifically for weight loss.
If you’re hoping to avoid injections while using GLP-1 medications, understanding what’s actually available versus what’s in development helps set realistic expectations. While injectable tirzepatide and semaglutide dominate the weight loss market, researchers are actively working on oral formulations that could provide needle-free alternatives.
The current reality is that injectable semaglutide and tirzepatide remain far more effective than oral options for weight loss. However, for people with needle phobia or strong injection aversion, oral semaglutide offers a less effective but viable alternative.
TrimRx provides access to injectable compounded medications with patient support to make injections as comfortable as possible.
Is Oral Tirzepatide Available?
No, oral tirzepatide is not currently available in any approved form. Neither Eli Lilly (the manufacturer of Mounjaro and Zepbound) nor any compounding pharmacy can legally provide oral tirzepatide at this time.
Why Oral Tirzepatide Doesn’t Exist Yet:
Pharmaceutical Challenge: GLP-1 medications like tirzepatide and semaglutide are large peptide molecules that break down quickly in the digestive system. When you swallow a peptide medication, stomach acid and digestive enzymes destroy most of the active ingredient before it can reach your bloodstream.
The Numbers:
- Injectable tirzepatide: Nearly 100% bioavailability (all medication reaches bloodstream)
- Oral peptides without enhancement: Less than 1% bioavailability
- This means you’d need 100 times more medication in oral form to match injection effectiveness
Technical Barriers: Creating an oral version requires solving multiple problems:
- Protecting the peptide from stomach acid
- Preventing breakdown by digestive enzymes
- Getting the large molecule through intestinal walls
- Maintaining therapeutic drug levels
- Doing all this at a reasonable cost
Current Development Status:
Eli Lilly has not publicly announced advanced clinical trials for oral tirzepatide. While the company likely has research programs exploring oral delivery, no oral tirzepatide formulation has entered Phase 3 trials (the final stage before FDA approval).
Timeline Estimates: Based on typical pharmaceutical development, if Eli Lilly started Phase 1 trials for oral tirzepatide today, FDA approval would likely be 5-7 years away at minimum. No such trials have been announced.
What About “Oral Tirzepatide” You See Online?
Red Flags and Scams:
Some websites or social media sellers claim to offer “oral tirzepatide” or “tirzepatide capsules.” These are not legitimate for several reasons:
- No FDA-Approved Form Exists: Any oral tirzepatide being sold is either fake, contains different ingredients, or is completely fraudulent.
- Compounding Pharmacies Cannot Make It: FDA regulations don’t permit compounding of oral tirzepatide because no approved oral formulation exists to compound from.
- Research Chemicals: Some sellers offer tirzepatide “for research purposes only,” which are not pharmaceutical-grade and not safe for human consumption.
- Counterfeit Medications: Scammers capitalize on people’s desire to avoid injections by selling fake or mislabeled products.
Never buy “oral tirzepatide” from:
- Online marketplaces
- Social media sellers
- International pharmacies claiming special formulations
- Research chemical suppliers
- Any source that doesn’t require a prescription
What You Can Actually Get:
If you want GLP-1 medication without injections, your only legitimate option currently is oral semaglutide (Rybelsus), which we’ll cover in detail below.
For people who need tirzepatide specifically, injectable tirzepatide remains the only safe and effective option. The injections use very small needles and subcutaneous administration (under the skin, not into muscle), making them much less uncomfortable than most people expect.
Current Oral GLP-1 Medications on the Market
Only one oral GLP-1 medication has FDA approval: semaglutide (Rybelsus). Understanding how this medication works helps explain why oral GLP-1s are challenging to develop.
Rybelsus (Oral Semaglutide):
What It Is: Rybelsus is the only FDA-approved oral GLP-1 medication. It contains the same active ingredient as Ozempic and Wegovy (semaglutide) but in a tablet form with a special absorption enhancer.
FDA Approval Status:
- Approved: September 2019
- Indication: Type 2 diabetes management
- NOT approved for weight loss specifically
- Manufacturer: Novo Nordisk
Available Doses:
- 3 mg (starting dose)
- 7 mg (maintenance dose)
- 14 mg (maximum dose)
How Rybelsus Works:
SNAC Technology: Rybelsus uses a compound called SNAC (salcaprozate sodium) to help semaglutide absorb through the stomach lining. SNAC temporarily increases the stomach’s pH and makes the stomach wall more permeable, allowing some semaglutide to pass into the bloodstream before digestive enzymes break it down.
Bioavailability: Even with SNAC technology, oral semaglutide has only 0.4-1% bioavailability compared to injectable semaglutide. This means you absorb less than 1% of the medication you swallow, which is why oral doses are much higher than injectable doses.
Strict Administration Requirements:
Rybelsus has very specific instructions that must be followed exactly:
- Take on empty stomach (first thing in morning before eating or drinking)
- With no more than 4 ounces of plain water
- Wait 30 minutes before eating, drinking, or taking other medications
- Swallow whole (don’t crush, chew, or split)
Breaking these rules dramatically reduces absorption and effectiveness.
Weight Loss Results with Rybelsus:
While not FDA-approved for weight loss, clinical trials showed:
- 3 mg dose: 1-2% body weight loss
- 7 mg dose: 2-3% body weight loss
- 14 mg dose: 3-5% body weight loss
Compare to injectable semaglutide (Wegovy):
- 2.4 mg weekly injection: 10-15% body weight loss
The difference: Injectable semaglutide produces 3-5 times more weight loss than oral semaglutide at maximum doses.
Why Doctors Don’t Prescribe Rybelsus for Weight Loss:
Most weight loss physicians don’t recommend Rybelsus for weight loss because:
- Much less effective than injectable options
- Strict dosing requirements reduce real-world effectiveness
- Higher cost for significantly lower results
- Not covered by insurance for weight loss indication
- Injectable options produce better outcomes with once-weekly dosing versus daily tablets
Who Uses Rybelsus: Primarily patients with type 2 diabetes who:
- Have severe needle phobia preventing injectable use
- Want to try a GLP-1 but refuse injections
- Are starting GLP-1 therapy and testing tolerance before committing to injections
- Have mild diabetes not requiring aggressive management
Cost Comparison:
- List Price: Approximately $900-$1,000 per month
- With Insurance: $25-$300 depending on coverage (usually for diabetes, not weight loss)
- Without Insurance: Full price unless using manufacturer coupon
For comparison, compounded injectable semaglutide costs $199/month and produces far superior weight loss results.
Other “Oral GLP-1” Options:
Liraglutide (Saxenda):
- Injectable only (not oral)
- Daily injections required
- Older GLP-1 medication
- Less effective than semaglutide or tirzepatide
- Not available in oral form
Dulaglutide (Trulicity):
- Injectable only (not oral)
- Once-weekly injection
- Primarily for diabetes
- Not available in oral form
Exenatide (Byetta, Bydureon):
- Injectable only (not oral)
- Twice daily or once weekly depending on formulation
- Older GLP-1 medication
- Not available in oral form
Bottom Line on Current Options:
If you want an oral GLP-1 medication right now, Rybelsus is your only option, but it’s significantly less effective for weight loss than injections. Most people achieve better results by overcoming injection anxiety rather than settling for less effective oral options.
How Oral GLP-1s Work Compared to Injections
Understanding the differences between oral and injectable delivery helps explain why injections remain the gold standard for weight loss.
Injectable GLP-1 Mechanism:
Subcutaneous Injection: When you inject semaglutide or tirzepatide under the skin:
- Medication forms depot: Creates a small reservoir under the skin
- Slow absorption: Gradually releases into bloodstream over days
- Steady drug levels: Maintains consistent therapeutic concentration for one week
- Nearly complete bioavailability: Almost all medication reaches systemic circulation
- Predictable dosing: Precise amount of medication absorbed
Why This Works So Well:
- Bypasses digestive system completely
- No breakdown by stomach acid or enzymes
- Consistent absorption across patients
- Once-weekly dosing maintains stable drug levels
- Can use relatively small doses for maximum effect
Oral GLP-1 Mechanism (Rybelsus):
Tablet Absorption Process: When you swallow Rybelsus:
- SNAC creates temporary window: Absorption enhancer raises stomach pH and increases permeability
- Limited absorption time: 30-minute window before medication moves to small intestine
- Most medication destroyed: Stomach acid and enzymes break down 99%+ of semaglutide
- Small amount reaches bloodstream: Less than 1% absorbed
- Rapid clearance: Daily dosing needed to maintain any therapeutic level
Why This Is Challenging:
- Requires much higher doses (14 mg oral vs 2.4 mg injectable weekly)
- Strict timing requirements
- Variable absorption between patients
- Food, beverages, and other medications interfere with absorption
- Still less effective despite higher doses
Pharmacokinetic Comparison:
| Metric | Injectable Semaglutide | Oral Semaglutide (Rybelsus) |
| Bioavailability | ~100% | <1% |
| Dosing Frequency | Once weekly | Once daily |
| Time to Peak Level | 1-3 days | 1 hour |
| Half-Life | 7 days | N/A (cleared daily) |
| Steady State | 4-5 weeks | Does not reach traditional steady state |
| Dose Required | 2.4 mg/week for weight loss | 14 mg/day (much higher) |
Absorption Challenges for Oral Peptides:
Size Matters: GLP-1 medications are large molecules (peptides with 30-40 amino acids). Large molecules don’t easily cross intestinal walls designed to absorb small nutrients.
Digestive Breakdown: Your digestive system is designed to break down proteins (including peptides) into amino acids. GLP-1 medications look like food to your digestive enzymes.
Stomach Acid: pH 1-2 in stomach denatures protein structure, destroying medication before it can be absorbed.
First-Pass Metabolism: Even if medication reaches the small intestine, the liver metabolizes much of what does get absorbed before it can reach systemic circulation.
Why Injections Are More Effective:
For Weight Loss Specifically:
Injectable GLP-1s produce superior weight loss because:
- Higher Effective Dose: 100% of injected medication becomes available vs <1% of oral medication
- Sustained Drug Levels: Once-weekly injection maintains appetite suppression consistently
- Stronger Brain Effects: Higher blood levels better activate appetite centers in the brain
- Gastric Emptying: More pronounced slowing of stomach emptying with injectable doses
- Consistent Results: Less variability in absorption leads to more predictable outcomes
Patient Adherence:
Surprisingly, many patients find weekly injections easier than daily tablets because:
- Don’t have to remember medication every morning
- No food/drink restrictions throughout the week
- Missing one day of oral medication can significantly impact effectiveness
- Weekly routine easier to maintain than strict daily morning ritual
When Oral Might Be Preferred:
Despite lower effectiveness, oral GLP-1s may be appropriate for:
- Severe needle phobia with no improvement after therapy/counseling
- Religious or cultural objections to injections
- Clotting disorders making injections risky
- Skin conditions affecting injection sites
- Patients starting GLP-1 therapy who want to test tolerability
- Mild type 2 diabetes not requiring aggressive treatment
For most weight loss patients, injectable options offer significantly better results even when accounting for injection discomfort.
Effectiveness: Oral vs Injectable Options
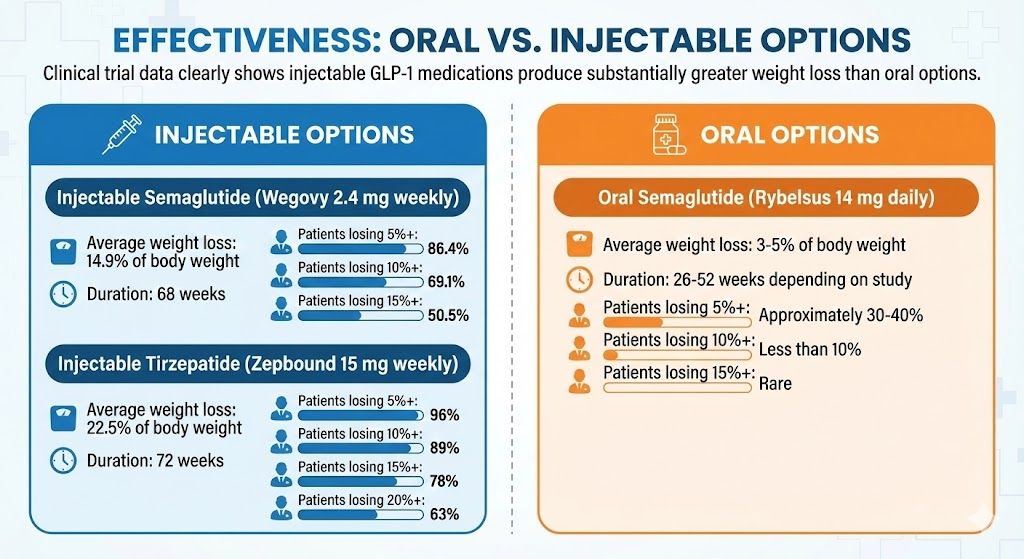
Clinical trial data clearly shows injectable GLP-1 medications produce substantially greater weight loss than oral options.
Weight Loss Comparison:
Injectable Semaglutide (Wegovy 2.4 mg weekly):
- Average weight loss: 14.9% of body weight
- Duration: 68 weeks
- Patients losing 5%+: 86.4%
- Patients losing 10%+: 69.1%
- Patients losing 15%+: 50.5%
Injectable Tirzepatide (Zepbound 15 mg weekly):
- Average weight loss: 22.5% of body weight
- Duration: 72 weeks
- Patients losing 5%+: 96%
- Patients losing 10%+: 89%
- Patients losing 15%+: 78%
- Patients losing 20%+: 63%
Oral Semaglutide (Rybelsus 14 mg daily):
- Average weight loss: 3-5% of body weight
- Duration: 26-52 weeks depending on study
- Patients losing 5%+: Approximately 30-40%
- Patients losing 10%+: Less than 10%
- Patients losing 15%+: Rare
Real-World Weight Loss Examples:
Starting Weight: 250 pounds
| Medication | Average Loss | Final Weight | Pounds Lost |
| Injectable Tirzepatide | 22.5% | 194 lbs | 56 lbs |
| Injectable Semaglutide | 14.9% | 213 lbs | 37 lbs |
| Oral Semaglutide | 4% | 240 lbs | 10 lbs |
Starting Weight: 200 pounds
| Medication | Average Loss | Final Weight | Pounds Lost |
| Injectable Tirzepatide | 22.5% | 155 lbs | 45 lbs |
| Injectable Semaglutide | 14.9% | 170 lbs | 30 lbs |
| Oral Semaglutide | 4% | 192 lbs | 8 lbs |
Why Such a Big Difference?
The 3-5x difference in weight loss comes from:
Bioavailability Gap: Less than 1% of oral semaglutide reaches your bloodstream versus nearly 100% of injectable forms. Even though oral doses are much higher, the amount that actually works in your body is far lower.
Drug Level Consistency: Injectable medications maintain steady therapeutic levels for a full week. Oral medications have peaks and valleys with mostly subtherapeutic levels between doses.
Appetite Suppression Duration: Weekly injections provide continuous appetite reduction. Daily oral medication provides limited suppression that wears off between doses (especially if you miss a day or don’t follow strict timing rules).
Gastric Effects: Higher systemic drug levels from injections produce stronger effects on stomach emptying and satiety signaling.
Clinical Study Data:
PIONEER Trials (Oral Semaglutide):
PIONEER 1 (Oral Semaglutide vs Placebo):
- 14 mg oral semaglutide: 4.2 kg (9.3 pounds) average weight loss
- Placebo: 0.8 kg (1.8 pounds) average weight loss
- Duration: 26 weeks
- Conclusion: Modest weight loss, far below injectable results
PIONEER 4 (Oral vs Injectable Semaglutide Direct Comparison):
- 14 mg oral semaglutide daily: 3.7 kg (8.2 pounds)
- 1.0 mg injectable semaglutide weekly: 5.0 kg (11 pounds)
- Even at lower injectable dose, injections produced 35% more weight loss
- Duration: 26 weeks
Real-World Effectiveness:
Doctors report that real-world results with Rybelsus are often worse than clinical trials because:
Adherence Challenges:
- Must take on empty stomach first thing in morning
- 30-minute wait before eating or drinking anything else
- Patients frequently forget or break the rules
- Each missed or improperly taken dose reduces effectiveness
Food Interference:
- Coffee with oral medication: Dramatically reduces absorption
- Taking with food: Almost completely prevents absorption
- Taking with other medications: May interfere with absorption
Patient Expectations: Many patients expect oral semaglutide to work as well as injections, leading to disappointment and discontinuation.
Who Succeeds with Oral Semaglutide:
The small number of patients who achieve meaningful weight loss with Rybelsus typically:
- Follow dosing instructions perfectly every single day
- Have structured morning routines
- Combine medication with significant lifestyle changes
- Have realistic expectations (5-10 pounds, not 30-50 pounds)
- Use it as a stepping stone before transitioning to injections
Bottom Line on Effectiveness:
For serious weight loss (15-50+ pounds), injectable GLP-1 medications are dramatically more effective. Oral semaglutide may help with 5-15 pounds of weight loss if you’re extremely compliant with dosing instructions, but most people achieve better results with injectable options despite initial injection hesitation.
Side Effects and Safety Profile
Oral and injectable GLP-1 medications share similar side effects, though the frequency and severity differ due to absorption differences.
Common Side Effects (Both Oral and Injectable):
Gastrointestinal Issues:
These are the most common side effects for all GLP-1 medications:
Nausea:
- Oral semaglutide (Rybelsus): 11-20% of patients
- Injectable semaglutide (Wegovy): 44% of patients
- Injectable tirzepatide (Zepbound): 30-37% of patients
Why the difference: Lower bioavailability of oral medication means less systemic exposure, potentially resulting in fewer GI side effects. However, this comes at the cost of much lower effectiveness.
Diarrhea:
- Oral semaglutide: 8-12% of patients
- Injectable semaglutide: 30% of patients
- Injectable tirzepatide: 19-23% of patients
Vomiting:
- Oral semaglutide: 5-8% of patients
- Injectable semaglutide: 24% of patients
- Injectable tirzepatide: 9-17% of patients
Abdominal Pain:
- Oral semaglutide: 6-10% of patients
- Injectable semaglutide: 20% of patients
- Injectable tirzepatide: 8-11% of patients
Unique to Oral Semaglutide:
SNAC-Related Side Effects:
The absorption enhancer (SNAC) in Rybelsus can cause additional issues:
Stomach Irritation:
- Heartburn or acid reflux
- Stomach discomfort or pain
- Gastrointestinal upset beyond typical GLP-1 effects
- May worsen pre-existing reflux or gastritis
Oral Medication Compliance Issues:
- Difficulty remembering daily dosing
- Frustration with strict timing requirements
- Reduced effectiveness if rules not followed perfectly
Injectable-Specific Side Effects:
Injection Site Reactions:
- Redness, swelling, or itching where you inject
- Occurs in 5-10% of patients
- Usually mild and resolves within days
- Rotating injection sites minimizes risk
- Not possible with oral medications (obvious advantage)
Serious Side Effects (Both Forms):
These rare but serious risks apply to both oral and injectable GLP-1 medications:
Pancreatitis:
- Severe abdominal pain radiating to back
- Risk: Less than 1% with any GLP-1 medication
- Requires immediate discontinuation
- Equal risk with oral or injectable
Thyroid Tumors (Black Box Warning):
- Based on animal studies (not confirmed in humans)
- Contraindicated with personal or family history of medullary thyroid carcinoma
- MEN 2 syndrome is absolute contraindication
- Warning applies to all GLP-1 receptor agonists
Gallbladder Problems:
- Gallstones, cholecystitis
- Related to rapid weight loss more than medication itself
- More common with injectable forms due to greater weight loss
Kidney Issues:
- Dehydration from vomiting/diarrhea can affect kidney function
- Monitor hydration carefully
- Report decreased urination or swelling
Hypoglycemia:
- Low blood sugar if combined with insulin or sulfonylureas
- Less common with GLP-1 medications alone
- Diabetic patients need monitoring
Safety Comparison:
Oral Semaglutide May Be Safer For:
- People with bleeding disorders (no injection risks)
- Patients with skin conditions affecting multiple injection sites
- Those with psychological trauma related to needles
Injectable Forms May Be Safer For:
- People with gastroesophageal reflux disease (GERD)
- Those with gastroparesis or slow stomach emptying
- Patients who struggle with daily medication adherence (weekly dosing reduces missed doses)
Contraindications (All GLP-1 Medications):
Do not use oral or injectable GLP-1 medications if you have:
- Personal or family history of medullary thyroid carcinoma
- Multiple endocrine neoplasia syndrome type 2 (MEN 2)
- History of severe GLP-1 allergic reaction
- Pregnancy or planning pregnancy
- History of pancreatitis (relative contraindication, discuss with provider)
Managing Side Effects:
For Oral Semaglutide:
- Take with small amount of water only (no coffee, tea, juice)
- Wait full 30 minutes before eating to maximize absorption and minimize nausea
- Start with lowest dose (3 mg) and escalate slowly
- Report persistent stomach pain (may be SNAC irritation)
For Injectable GLP-1s:
- Start with lowest dose and increase gradually
- Inject before bed to sleep through initial nausea
- Eat smaller, more frequent meals
- Stay well-hydrated
- Ask provider about anti-nausea medication
- Rotate injection sites to prevent skin reactions
Discontinuation Rates:
Due to Side Effects:
- Oral semaglutide: 4-7% discontinuation rate
- Injectable semaglutide: 6.9% discontinuation rate
- Injectable tirzepatide: 6.2% discontinuation rate
Despite higher side effect rates, injectable medications don’t have significantly higher discontinuation rates because the benefits outweigh temporary discomfort for most patients.
Cost Comparison: Oral vs Injectable GLP-1s
Understanding the full cost picture helps determine if oral medication’s convenience justifies its lower effectiveness.
Brand-Name Costs (Without Insurance):
Oral Semaglutide (Rybelsus):
- List Price: $900-$1,000 per month
- 30-day supply (30 tablets)
- Must take daily
- Annual cost: $10,800-$12,000
Injectable Semaglutide (Wegovy):
- List Price: $1,349 per month
- 4-5 weekly injections per pack
- Weekly dosing
- Annual cost: $16,188
Injectable Tirzepatide (Zepbound):
- List Price: $1,069 per month
- 4 weekly injections per pack
- Weekly dosing
- Annual cost: $12,828
With Insurance Coverage:
Oral Semaglutide:
- More likely to be covered for diabetes
- Weight loss coverage varies
- Copay: $25-$300/month with insurance
- Prior authorization usually required
Injectable Semaglutide (Wegovy):
- Covered by some insurance for weight loss
- Copay: $25-$300/month with insurance
- Extensive prior authorization requirements
- May require failed weight loss attempts first
Injectable Tirzepatide (Zepbound):
- Newer to market, less insurance coverage for weight loss
- Copay: $25-$300/month with insurance
- Even more restrictive prior authorization
- Many plans don’t cover yet for weight loss
Compounded Injectable Options:
Compounded Semaglutide:
- TrimRx price: $199/month with annual commitment
- Other providers: $199-$599/month
- No insurance coverage but HSA/FSA eligible
- Annual cost: $2,388-$7,188
Compounded Tirzepatide:
- TrimRx price: $349/month with annual commitment
- Other providers: $349-$699/month
- No insurance coverage but HSA/FSA eligible
- Annual cost: $4,188-$8,388
No Compounded Oral Options: Compounding pharmacies cannot create oral semaglutide because the SNAC absorption technology is proprietary and patented. Only Novo Nordisk can produce Rybelsus.
Cost-Effectiveness Analysis:
Cost per Pound Lost (Estimated):
Oral Semaglutide (Rybelsus):
- Average weight loss: 10 pounds (for 250 lb person)
- Cost: $900-$1,000/month for 6 months = $5,400-$6,000
- Cost per pound lost: $540-$600
Injectable Semaglutide (Compounded from TrimRx):
- Average weight loss: 37 pounds (for 250 lb person)
- Cost: $199/month for 16 months = $3,184
- Cost per pound lost: $86
Injectable Tirzepatide (Compounded from TrimRx):
- Average weight loss: 56 pounds (for 250 lb person)
- Cost: $349/month for 18 months = $6,282
- Cost per pound lost: $112
Value Comparison:
| Medication | Monthly Cost | Effectiveness | Cost per % Body Weight Lost | Value Rating |
| Oral Semaglutide (Brand) | $900-$1,000 | 3-5% loss | $200-$250 per % | Poor |
| Injectable Semaglutide (Compounded) | $199 | 14.9% loss | $13 per % | Excellent |
| Injectable Tirzepatide (Compounded) | $349 | 22.5% loss | $16 per % | Excellent |
| Injectable Semaglutide (Brand) | $1,349 | 14.9% loss | $91 per % | Poor (unless insurance covers) |
Hidden Costs:
Oral Semaglutide:
- No injection supplies needed (saves $20-30/month)
- May require acid reflux medication if SNAC causes irritation
- Potential need for additional weight loss interventions if not effective
Injectable Medications:
- Injection supplies usually included or inexpensive
- Sharps container ($5-10 one-time)
- Potential anti-nausea medication ($10-30/month if needed)
Insurance Variables:
If your insurance covers Rybelsus with a $25-$50 copay, it may seem like an attractive option. However, consider:
Questions to Ask:
- Is coverage for type 2 diabetes only, or also weight loss?
- What prior authorization requirements exist?
- How long will coverage continue?
- What happens if it doesn’t work well?
Many patients who start with oral semaglutide due to insurance coverage eventually switch to compounded injectables when results disappoint.
Bottom Line on Cost:
Oral semaglutide costs about the same as brand-name injectables but delivers only 20-30% of the weight loss results. For cash-pay patients, compounded injectable semaglutide at $199/month provides dramatically better value than oral options costing $900-$1,000/month.
Who Should Consider Oral GLP-1 Options
Despite lower effectiveness, oral semaglutide makes sense for a specific subset of patients.
Good Candidates for Oral Semaglutide:
- People with Severe Needle Phobia
If you have genuine needle phobia (not just hesitation) that hasn’t improved with:
- Cognitive behavioral therapy
- Exposure therapy
- Counseling or support
- Using the smallest gauge needles
Then oral medication may be your only option to access GLP-1 therapy. Some weight loss (3-5%) is better than no intervention.
- Medical Conditions Preventing Injections
Certain health conditions make injections risky:
- Severe bleeding disorders (hemophilia, severe thrombocytopenia)
- Anticoagulation therapy with high bleeding risk
- Skin conditions affecting multiple injection sites (psoriasis, eczema, scarring)
- Lymphedema affecting typical injection areas
- Religious or Cultural Considerations
Some individuals have religious or cultural objections to:
- Self-injection practices
- Specific injection methods
- Needle use for non-medical emergencies
If these beliefs are deeply held, oral medication provides an alternative while respecting personal values.
- Patients Starting GLP-1 Therapy
Some doctors prescribe oral semaglutide as a “test run” for patients who:
- Want to assess GLP-1 tolerability before committing to injections
- Have concerns about nausea and want to try a lower-exposure option first
- Plan to transition to injections after demonstrating good tolerance
This strategy can build confidence, though starting directly with injectable therapy (at the lowest dose) often works just as well.
- Mild Weight Loss Goals
If you only need to lose 10-20 pounds and:
- Have time to lose weight gradually
- Are committed to strict dietary changes alongside medication
- View medication as a small boost to lifestyle efforts
- Don’t mind daily oral medication routines
Oral semaglutide might provide enough support, though injectable options would still work better.
- Type 2 Diabetics Needing Mild Glucose Control
If your primary goal is blood sugar management (not significant weight loss) and:
- A1C is mildly elevated (7.0-8.0%)
- Diet and metformin aren’t quite enough
- You refuse injectable medications
- Modest additional glucose control would help
Rybelsus serves its FDA-approved indication well in this context.
Poor Candidates for Oral Semaglutide:
- People Seeking Significant Weight Loss
If you need to lose 30+ pounds, oral semaglutide will likely disappoint. The 3-5% average weight loss won’t meet your goals, and you’ll waste money and time.
Better option: Start with injectable semaglutide or tirzepatide to maximize results.
- Patients with GERD or Gastroparesis
The SNAC absorption enhancer can irritate stomach lining and worsen:
- Gastroesophageal reflux disease
- Chronic gastritis
- Delayed stomach emptying
- Peptic ulcers
Injectable options don’t have these issues.
- People with Chaotic Morning Routines
Rybelsus requires:
- Waking at consistent times
- Taking medication before anything else (including coffee)
- Waiting 30 full minutes before eating or drinking
- No other medications during that 30-minute window
If you can’t commit to this strict routine every single day, oral semaglutide won’t work effectively. Weekly injections are actually more convenient for people with variable schedules.
- Cost-Conscious Patients Paying Cash
At $900-$1,000/month for minimal results, oral semaglutide is poor value for cash-pay patients. Compounded injectable semaglutide ($199/month) costs 80% less and produces 3-5x more weight loss.
- Impatient Patients
If you want to see results quickly (within 2-3 months), oral semaglutide’s modest effects will frustrate you. Injectable options produce noticeable results much faster.
Questions to Ask Yourself:
Before Choosing Oral Semaglutide:
- Have I tried injectable GLP-1s? If not, how do you know you can’t tolerate them?
- Is my needle fear rational or manageable? Most people find GLP-1 injections far less uncomfortable than anticipated once they try.
- Am I willing to follow strict daily dosing rules? Missing doses or breaking rules makes oral medication even less effective.
- Are my weight loss goals modest? If you need to lose 10-15 pounds, oral may suffice. For 30-50+ pounds, injectable is better.
- What’s my budget? If paying cash, compounded injectables cost 80% less than oral brand-name options.
- Does my insurance cover it? If insurance covers Rybelsus with low copay, it might be worth trying despite lower effectiveness.
Transitioning from Oral to Injectable:
Many patients start with oral semaglutide then switch to injectable forms when:
- Weight loss plateaus at 5-10 pounds
- Results are disappointing
- Tired of daily medication routine
- Built confidence with GLP-1 therapy
- Insurance or financial situation changes
Switching Process:
- Stop oral semaglutide
- Wait one week
- Start injectable semaglutide at 0.25 mg weekly (regardless of oral dose)
- Escalate dose according to standard protocol
Most people successfully transition and appreciate the improved results with weekly injections.
The Future of Oral Tirzepatide Development
While oral tirzepatide isn’t available now, pharmaceutical companies are actively researching oral GLP-1 and GIP/GLP-1 formulations.
Eli Lilly’s Research Direction:
Eli Lilly has not publicly announced Phase 3 trials for oral tirzepatide, but the company’s research likely includes:
Potential Approaches:
- SNAC Technology Licensing
- Novo Nordisk owns patents on SNAC (used in Rybelsus)
- Eli Lilly would need to license technology or develop alternatives
- Patent protections last until 2030s
- Licensing agreements could accelerate development
- Alternative Absorption Enhancers
- Other permeation enhancers exist (sodium N-[8-(2-hydroxybenzoyl)amino]caprylate)
- May offer similar benefits without patent conflicts
- Requires extensive safety and efficacy testing
- Nanoparticle Delivery Systems
- Encapsulating peptides in protective nanoparticles
- Allows passage through stomach without degradation
- Several companies researching this technology
- Still in early development stages
- Modified Peptide Structures
- Chemically modifying tirzepatide to resist digestion
- Could improve oral bioavailability
- Must maintain therapeutic effects while changing structure
- Challenging scientific problem
- Sublingual or Buccal Delivery
- Absorption through mouth tissues instead of digestive system
- Bypasses stomach acid entirely
- Some peptides absorb well through oral mucosa
- Limited capacity for large molecules like tirzepatide
Development Timeline Reality:
Pharmaceutical Development Stages:
Phase 1: Safety Testing (1-2 years)
- Small group of healthy volunteers
- Tests safety, dosing, side effects
- Determines if oral formulation is safe enough to continue
Phase 2: Efficacy Testing (2-3 years)
- Patients with target condition
- Tests if oral formulation actually works
- Determines optimal dosing
- Many drugs fail at this stage
Phase 3: Large-Scale Trials (2-4 years)
- Thousands of patients
- Proves effectiveness and safety at scale
- Required for FDA approval
- Most expensive phase
FDA Review and Approval (1-2 years)
- Submission of trial data
- FDA review process
- Potential requests for additional information
- Final approval and launch
Total Timeline: 6-11 years from starting Phase 1 to FDA approval
Current Status (As of 2025):
No oral tirzepatide formulation has been announced in Phase 3 trials. If Eli Lilly started Phase 1 today, FDA approval would likely arrive around 2030-2035 at the earliest.
Alternative Approaches Being Researched:
Other Companies’ Oral GLP-1 Programs:
Several pharmaceutical and biotech companies are developing oral GLP-1 or dual agonist medications:
Pfizer:
- Developing oral GLP-1 receptor agonist (danuglipron)
- Different molecule than semaglutide or tirzepatide
- Phase 2 trials showed promise but also significant GI side effects
- Still years from potential approval
Novo Nordisk:
- Researching higher-dose oral semaglutide formulations
- Exploring oral versions of other GLP-1 medications in pipeline
- Owns SNAC technology, giving them advantage
Veru Inc.:
- Developing oral GLP-1 using different technology
- Early-stage research
- At least 5-7 years from approval if successful
Structure Therapeutics:
- Oral GLP-1 receptor agonist in development
- Early clinical trials
- Results not yet published
Realistic Expectations:
What’s Likely by 2030:
- Improved oral semaglutide formulations (higher doses, better absorption)
- Possibly oral tirzepatide if development accelerates
- Other oral GLP-1 medications from competing companies
- Better absorption technologies
What’s Unlikely by 2030:
- Oral GLP-1 medications as effective as current injections
- Oral medications without strict dosing requirements
- Oral options significantly cheaper than injections
The Physics Problem:
Even with better technology, oral peptides face fundamental limitations:
- Large molecules don’t easily cross intestinal barriers
- Digestive system will always break down some medication
- First-pass liver metabolism reduces bioavailability
- Perfect oral bioavailability is likely impossible for peptides this size
Most Likely Outcome:
Future oral tirzepatide will probably:
- Require higher doses than injectable (like Rybelsus does now)
- Have strict administration requirements
- Be less effective than injectable versions
- Cost similar to or more than current brand-name injectable options
- Serve niche population unable or unwilling to inject
Should You Wait for Oral Tirzepatide?
If you need to lose weight now: Don’t wait 5-10 years for oral tirzepatide. Current injectable options are highly effective and well-tolerated by most people.
If you have mild needle hesitation: Try current injectable medications. Most people find the small needles far less uncomfortable than anticipated. Waiting years for a less effective option doesn’t make sense.
If you have severe needle phobia: Consider Rybelsus (oral semaglutide) as an imperfect but available option now. Don’t wait years hoping for oral tirzepatide.
The Injection Reality:
Modern GLP-1 injections use:
- 32-gauge needles (thinner than a human hair)
- Very short needles (4-6mm)
- Subcutaneous injection (under skin, not into muscle)
- Spring-loaded pens that hide the needle
- Once-weekly dosing instead of daily
Most patients report injections are:
- Virtually painless
- Far less scary than anticipated
- Much easier than daily oral medication routines
- Worth it for superior results
Frequently Asked Questions
Is oral tirzepatide currently available? No, oral tirzepatide is not currently available in any approved form. Eli Lilly has not announced advanced clinical trials for oral tirzepatide. The only available oral GLP-1 medication is semaglutide (Rybelsus), which is FDA-approved for type 2 diabetes but not weight loss.
Can compounding pharmacies make oral tirzepatide? No, compounding pharmacies cannot legally create oral tirzepatide. The absorption technology needed to make oral GLP-1 medications work is proprietary and patented. Additionally, there is no approved oral formulation to compound from. Any source claiming to sell oral tirzepatide is not legitimate.
How effective is oral semaglutide (Rybelsus) for weight loss? Oral semaglutide produces modest weight loss of 3-5% of body weight on average, compared to 10-15% with injectable semaglutide (Wegovy) and 15-22% with injectable tirzepatide (Zepbound). For a 250-pound person, this means losing 8-12 pounds with oral versus 37-56 pounds with injectables.
Why don’t doctors prescribe Rybelsus for weight loss? Most weight loss physicians don’t recommend Rybelsus because it’s 3-5 times less effective than injectable options, requires strict daily dosing rules that reduce real-world effectiveness, and costs just as much as injectable medications while producing far inferior results. Injectable options provide better outcomes for patients seeking significant weight loss.
When will oral tirzepatide be available? If development started today, oral tirzepatide would likely require 6-11 years to reach FDA approval (typical pharmaceutical development timeline). As of 2025, Eli Lilly has not announced Phase 3 trials for oral tirzepatide, suggesting approval is at least 5-10 years away if the program proceeds successfully.
Are GLP-1 injections really painful? Most patients report GLP-1 injections are virtually painless. Modern injections use 32-gauge needles (extremely thin), inject under the skin rather than into muscle, and many people find them far less uncomfortable than anticipated. The once-weekly dosing is also more convenient than daily oral medications for many patients.
Can I buy oral tirzepatide online from other countries? No legitimate source can provide oral tirzepatide because it doesn’t exist in any approved form anywhere in the world. Any website or seller claiming to offer oral tirzepatide is either selling counterfeit products, mislabeled medications, or operating a scam. Do not purchase from these sources.
What if I absolutely cannot do injections? If medical or psychological reasons truly prevent injectable use, oral semaglutide (Rybelsus) is your only current FDA-approved option. While less effective than injections, it may provide modest weight loss (5-15 pounds) if you follow strict dosing instructions. Alternatively, consider working with a therapist to address needle phobia before ruling out more effective injectable options.
How much does oral semaglutide (Rybelsus) cost? Rybelsus costs approximately $900-$1,000 per month without insurance. With insurance coverage for diabetes (not typically covered for weight loss), copays range from $25-$300 monthly. This is similar to brand-name injectable medication costs but produces far less weight loss, making it poor value for cash-pay weight loss patients.
Can I switch from oral semaglutide to injectable tirzepatide? Yes, you can switch from oral semaglutide to injectable tirzepatide. Stop taking oral medication, wait one week, then start injectable tirzepatide at 2.5 mg weekly (starting dose). Your provider will guide the transition and determine appropriate dosing based on your previous medication and response.
Ready to start your weight loss journey with effective GLP-1 medications? While oral tirzepatide isn’t available, TrimRx offers affordable access to injectable compounded semaglutide ($199/month) and compounded tirzepatide ($349/month) with licensed medical oversight. Most patients find injections far more comfortable than expected and appreciate the superior weight loss results.
Transforming Lives, One Step at a Time
Keep reading

Sleep Apnea and Weight Loss: GLP-1 Benefits
Sleep apnea and obesity are so closely linked that weight loss is considered a first-line treatment for the condition, right alongside CPAP therapy. What’s…

GLP-1 for Metabolic Syndrome: Complete Guide
Metabolic syndrome isn’t a single disease. It’s a cluster of interconnected conditions that, when they appear together, dramatically raise your risk for type 2…

Endometriosis and Weight: Can GLP-1 Help?
Weight gain with endometriosis isn’t just about diet or willpower. The condition creates a hormonal and inflammatory environment that makes losing weight genuinely harder….

