Semaglutide to Tirzepatide: Switching Guide

Switching from semaglutide to tirzepatide is one of the most clinically supported medication transitions in GLP-1 weight loss treatment. You’re moving from a single-receptor medication (GLP-1 only) to a dual-receptor medication (GLP-1 plus GIP), which adds a second hormonal pathway that influences appetite, fat metabolism, and glucose regulation. Clinical trial data consistently shows tirzepatide producing greater average weight loss than semaglutide, making this switch particularly relevant for patients who’ve plateaued, want stronger results, or haven’t responded adequately to semaglutide alone.
This guide covers why people switch, how the transition works regardless of which brand you’re on, and what to realistically expect on the other side.
Why People Switch from Semaglutide to Tirzepatide
The reasons cluster into a few distinct categories.
Plateaued on maximum-dose semaglutide. This is the most common trigger. You’ve titrated up to 2 mg (Ozempic) or 2.4 mg (Wegovy), lost weight initially, and then stalled despite addressing diet, exercise, sleep, and medical factors. When you’ve exhausted the options within a single-receptor medication, adding a second receptor pathway through tirzepatide gives your body a genuinely new stimulus to respond to. Many patients who were stuck on semaglutide see renewed, significant weight loss after switching.
Appetite suppression has faded. Even at maximum dose, some patients find that semaglutide’s appetite control weakens over time. Food interest returns, portions creep up, and the effortless calorie reduction that characterized early treatment gradually disappears. Tirzepatide’s GIP receptor activity produces appetite suppression through mechanisms that semaglutide doesn’t access, which often restores strong food disinterest in patients who’d adapted to semaglutide’s effects.
Wanting a higher efficacy ceiling. Some patients research the data, see that tirzepatide produces roughly 5 to 7 percentage points more body weight loss on average than semaglutide, and want access to that additional potential. This is especially relevant for patients with a large amount of weight to lose who want to maximize their results.
Side effect profile differences. While both medications share similar GI side effects, individual responses vary. Some patients tolerate tirzepatide better than semaglutide, or vice versa. The only way to know is to try, and for patients whose semaglutide side effects have been problematic, switching is a reasonable exploration.
Understanding What Changes Pharmacologically
This isn’t a lateral move. You’re genuinely changing your treatment mechanism, and understanding the difference helps set expectations.
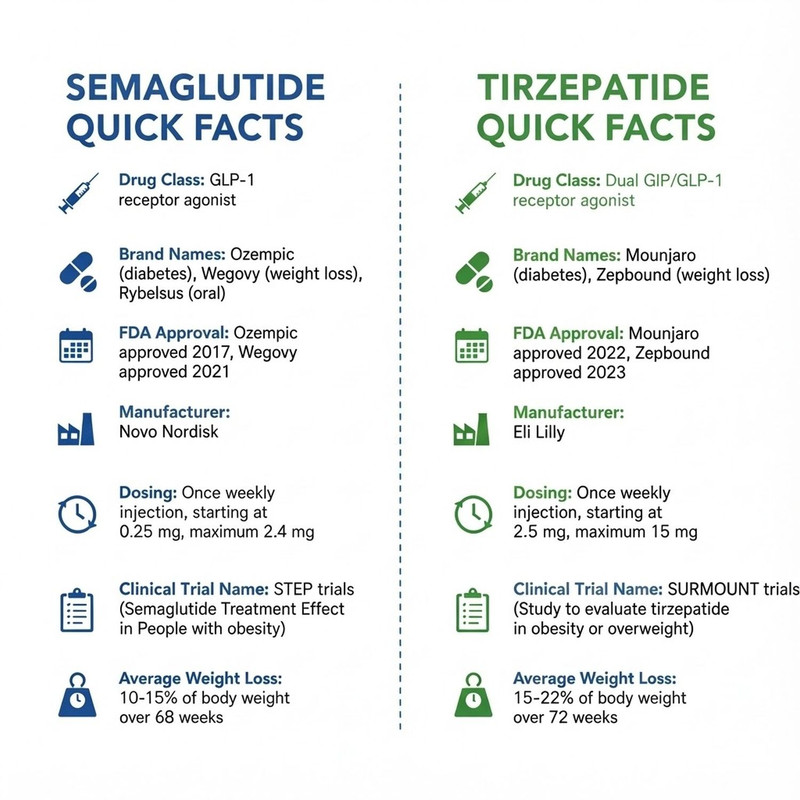
Semaglutide (Ozempic, Wegovy, or compounded) activates GLP-1 receptors exclusively. This slows gastric emptying, reduces appetite via hypothalamic signaling, improves insulin sensitivity, and reduces glucagon secretion. It’s effective, well-studied, and has strong real-world evidence behind it.
Tirzepatide (Mounjaro, Zepbound, or compounded) activates both GLP-1 and GIP receptors. The GLP-1 effects are similar to semaglutide. The added GIP activity influences fat cell metabolism, enhances insulin secretion in a glucose-dependent manner, and appears to modulate appetite through additional central nervous system pathways that GLP-1 alone doesn’t reach.
The practical result is that tirzepatide tends to produce stronger appetite suppression, greater fat loss relative to lean mass, and improved metabolic markers compared to semaglutide at their respective optimal doses. The SURPASS-2 trial (Frias et al., NEJM, 2021) directly compared tirzepatide to semaglutide 1 mg in patients with type 2 diabetes and found tirzepatide superior across all dose levels for both weight loss and glycemic control.
Which Brands Are Involved
Semaglutide is available as Ozempic (diabetes indication), Wegovy (weight management indication), and compounded semaglutide from telehealth providers like TrimRx.
Tirzepatide is available as Mounjaro (diabetes indication), Zepbound (weight management indication), and compounded tirzepatide.
The specific brand you switch from and to depends on your insurance coverage, your diagnosis, and your provider’s recommendation. The pharmacology is determined by the molecule, not the brand. Whether you’re going from Wegovy to Zepbound, Ozempic to Mounjaro, or compounded semaglutide to compounded tirzepatide, the clinical transition is the same.
How the Transition Works
The switch is straightforward. Take your last semaglutide injection on your regular day, then start tirzepatide the following week on that same day. No washout period. No bridging medications. No need to retitrate from the very bottom if your provider determines a higher starting dose is appropriate.
The starting dose on tirzepatide depends on your current semaglutide dose and how long you’ve been on it:
If you were on semaglutide 0.25 mg or 0.5 mg, start tirzepatide at 2.5 mg. Your GLP-1 exposure has been low, so standard onboarding applies.
If you were on semaglutide 1 mg, start tirzepatide at 2.5 mg or 5 mg. Many providers choose 5 mg here because your established GLP-1 tolerance means 2.5 mg would likely feel like a notable step down in appetite suppression.
If you were on semaglutide 1.7 mg to 2.4 mg (or Ozempic 2 mg), start tirzepatide at 5 mg. This is the most common starting point for patients switching from high-dose semaglutide. Some providers consider 7.5 mg for patients with excellent tolerability and no history of significant GI side effects, but 5 mg is the safer default.
From your starting dose, titration follows the standard tirzepatide schedule: increase by 2.5 mg every four weeks as tolerated, up to 15 mg. Your provider adjusts the pace based on your response and side effect profile.
What the First Few Weeks Feel Like
Patients who switch from semaglutide to tirzepatide commonly report a few distinct experiences.
Appetite suppression feels qualitatively different. On semaglutide, the dominant appetite effect for most people is early satiety during meals, feeling full quickly because gastric emptying is slowed. On tirzepatide, patients frequently describe an additional layer: reduced food interest between meals, fewer cravings, and less mental preoccupation with food. This broader suppression pattern likely reflects GIP receptor activity in appetite centers that GLP-1 alone doesn’t fully engage.
GI side effects may temporarily resurface. Your body is accustomed to GLP-1 stimulation, but GIP receptor activation is new. Mild nausea during the first few days, a brief shift in bowel patterns, or slight abdominal discomfort is common. These effects are generally milder and shorter-lived than what you experienced when first starting semaglutide, since one pathway is already familiar.
Consider this scenario: a patient switches from Wegovy 2.4 mg to tirzepatide 5 mg. Day one and two, they notice mild stomach discomfort and slightly less appetite than their recent baseline on Wegovy. Day three through five, GI symptoms fade. By week two, appetite suppression feels noticeably different, more like reduced food interest than just early fullness. They describe thinking about food less often, which they hadn’t experienced in months on semaglutide.
Energy and mood typically remain stable. Some patients report feeling slightly more energetic after the switch, possibly related to tirzepatide’s more pronounced effects on glucose stability. Others notice no change. Negative impacts on energy or mood are uncommon.
When Weight Loss Picks Up Again
If you’re switching because of a semaglutide plateau, realistic timing matters.
During the first two to four weeks, you’re adjusting to the new medication at a relatively low dose. Weight loss during this period is variable. Some patients see movement right away. Others don’t see significant changes until they’ve titrated up.
The inflection point for most patients comes between weeks four and eight, typically when they reach 7.5 mg or 10 mg. This is where tirzepatide’s dual mechanism starts operating at full strength for many people, and the kind of consistent, week-over-week weight loss that characterized your best months on semaglutide often returns.
By the three-month mark, most patients who switched from semaglutide have a clear picture of how their body responds to tirzepatide. The tirzepatide results timeline provides dose-by-dose benchmarks. The tirzepatide weight loss results cover the broader clinical data showing what’s achievable at higher doses.
If you haven’t seen improvement by the time you reach 10 mg (roughly two to three months in, depending on titration speed), it’s time to evaluate other factors: diet, exercise, sleep, medical conditions, and interfering medications. The medication is providing its pharmacological effect. Something else may be limiting your response.
Side Effect Management During the Transition
The same general strategies that work for any GLP-1 apply here, with a few transition-specific notes.
Eat smaller meals for the first one to two weeks at each new dose. Your GI system is adjusting to a new receptor stimulus, and large meals can overwhelm it. Prioritize lean protein and vegetables. High-fat foods slow digestion further and tend to worsen nausea when gastric emptying is already delayed. Keep hydration high. Dehydration worsens nearly every GI side effect. Aim for at least 64 ounces of water daily, more if you’re active. Consider injection timing. If you had a preferred injection time on semaglutide that worked well for managing side effects, try the same timing with tirzepatide as a starting point.
If you had sulfur burps on semaglutide, they may or may not occur on tirzepatide. Different molecule, potentially different GI response. The sulfur burps article covers remedies that apply regardless of which medication you’re taking.
Cost and Access Considerations
The brand you switch to (Mounjaro vs. Zepbound vs. compounded tirzepatide) depends on your insurance and budget.
If you have type 2 diabetes, Mounjaro is typically the easiest to get covered. If your primary indication is weight management, Zepbound is the FDA-appropriate product, though coverage varies significantly by plan.
For patients paying out of pocket or facing insurance barriers, compounded tirzepatide through TrimRx offers the same active ingredient at substantially lower cost. This is particularly relevant for patients switching from compounded semaglutide, since the transition can happen within the same telehealth provider without changing your care model.
If you were previously on compounded semaglutide through TrimRx, the switch to compounded tirzepatide is seamless from a logistical standpoint. Same provider platform, same home delivery model, different medication.
Making the Switch
Here’s the practical sequence:
Discuss the switch with your provider and agree on a tirzepatide starting dose. Secure your tirzepatide prescription and confirm it’s filled before your last semaglutide injection. Take your last semaglutide dose on your regular injection day. Start tirzepatide the following week on the same day. Monitor appetite, side effects, and weight over the first four weeks. Communicate with your provider about titration timing based on your tolerance and response.
If you’re ready to explore this transition, TrimRx’s intake quiz can connect you with a provider who manages semaglutide-to-tirzepatide switches regularly and can build a personalized titration plan based on your treatment history.
The data supports this switch for patients who’ve hit a ceiling on semaglutide. The dual mechanism genuinely adds something new, and for many patients, it’s the change that restarts meaningful progress.
This information is for educational purposes and is not medical advice. Consult with a healthcare provider before starting any medication. Individual results may vary.
Transforming Lives, One Step at a Time
Keep reading

How Much Protein Do You Need on Ozempic or Semaglutide
Most patients on Ozempic or semaglutide need between 100 and 140 grams of protein daily, significantly more than the average American consumes and more…

How Semaglutide Affects Your Hunger Hormones
Semaglutide works by changing the hormonal signals that control hunger, fullness, and food reward. Within the first few weeks of treatment, patients notice appetite…

Best Exercises to Do While on Ozempic or Semaglutide
The best exercises to do on Ozempic are the ones that preserve muscle, accelerate fat loss, and are sustainable enough to become a genuine…

